Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
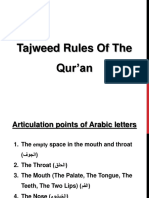
- Tajweed Rules of The Qur'anDokument25 SeitenTajweed Rules of The Qur'anridwanmdNoch keine Bewertungen
- Skills Test Unit 2 Test ADokument6 SeitenSkills Test Unit 2 Test ANastyusha Shapoval50% (2)
- Singaporian Math 1Dokument16 SeitenSingaporian Math 1nimanima50Noch keine Bewertungen
- DNS Chaitow Book 2Dokument6 SeitenDNS Chaitow Book 2Milos DjuricNoch keine Bewertungen
- Harry - Jimenz - Letter of Invitation PDFDokument1 SeiteHarry - Jimenz - Letter of Invitation PDFSampath Ravula100% (1)
- MRCPCH - ImmunisationDokument22 SeitenMRCPCH - Immunisationarooba sohaNoch keine Bewertungen
- Branchial Arch SyndromesDokument7 SeitenBranchial Arch SyndromesVita Dental PachucaNoch keine Bewertungen
- Stages of Evolution of ManDokument3 SeitenStages of Evolution of ManTristan Nialler100% (1)
- Axillary Node DissectionDokument71 SeitenAxillary Node DissectionKartik Kaistha100% (1)
- Syphilis During Pregnancy A Preventable Threat To Maternal-Fetal Health.Dokument12 SeitenSyphilis During Pregnancy A Preventable Threat To Maternal-Fetal Health.Andrés Felipe Jaramillo TorresNoch keine Bewertungen
- Bio Circulatory System WorksheetsDokument21 SeitenBio Circulatory System WorksheetsCraft City0% (1)
- Alphabet Adventures - Lyrics To The SongsDokument7 SeitenAlphabet Adventures - Lyrics To The SongsmaryleesunseriNoch keine Bewertungen
- Eizenberg S General Anatomy PDFDokument255 SeitenEizenberg S General Anatomy PDFNikita Leanne FernandesNoch keine Bewertungen
- MC ClureDokument27 SeitenMC ClureKotegardaNoch keine Bewertungen
- Lesson 9 MorphologyDokument51 SeitenLesson 9 Morphologymarta_srg100% (2)
- The Yearling: Study GuideDokument13 SeitenThe Yearling: Study GuideDaniel PalermoNoch keine Bewertungen
- Ancylostoma DuodenaleDokument2 SeitenAncylostoma DuodenaleBlessy BreganzaNoch keine Bewertungen
- Survival KitDokument8 SeitenSurvival KitedGarKazy77Noch keine Bewertungen
- Noun Proper and CommonDokument13 SeitenNoun Proper and CommonSurya BarrytappyNoch keine Bewertungen
- Strength Treatise by C A Sampson PDFDokument250 SeitenStrength Treatise by C A Sampson PDFJack100% (1)
- Hylestad Stave ChurchDokument3 SeitenHylestad Stave Churchsanjo93Noch keine Bewertungen
- Lower Extremity DisordersDokument14 SeitenLower Extremity DisordersJameson87Noch keine Bewertungen
- 4TH Periodical Test in English 2018-2019Dokument6 Seiten4TH Periodical Test in English 2018-2019Jhun Tandang100% (1)
- Chinese Metasoft: Home Products Da Liu Ren Ba Zi Qi Men Dun Jia Feng Shui Ze RiDokument1 SeiteChinese Metasoft: Home Products Da Liu Ren Ba Zi Qi Men Dun Jia Feng Shui Ze RiFingiel BluNoch keine Bewertungen
- Descriptive Words and PhrasesDokument39 SeitenDescriptive Words and PhrasesShukri Ayob100% (1)
- 2001 LamenessDokument112 Seiten2001 LamenessZozo Mostafa100% (1)
- Grammar Test 2Dokument1 SeiteGrammar Test 2Anikó AnikóNoch keine Bewertungen
- Identification of Invertebrate Taxonomic CharacterDokument6 SeitenIdentification of Invertebrate Taxonomic CharacterDaisy KavinskyNoch keine Bewertungen
- Gimme Ice Cream's BDSM ChecklistDokument20 SeitenGimme Ice Cream's BDSM Checklistgimmeicecream100% (3)
- Large Carnivore Conservation and Management (VetBooks - Ir) PDFDokument365 SeitenLarge Carnivore Conservation and Management (VetBooks - Ir) PDFFrancisco Cifuentes SilvaNoch keine Bewertungen