Das könnte Ihnen auch gefallen
- Canal Maintenance Shop Supervisor II: Passbooks Study GuideVon EverandCanal Maintenance Shop Supervisor II: Passbooks Study GuideNoch keine Bewertungen
- Senior Pump Operator: Passbooks Study GuideVon EverandSenior Pump Operator: Passbooks Study GuideNoch keine Bewertungen
- Ncert Form-2022Dokument6 SeitenNcert Form-2022suyashy143Noch keine Bewertungen
- Khairpur Medical College: Application FormDokument8 SeitenKhairpur Medical College: Application FormWaseem Abbas MangrioNoch keine Bewertungen
- Application Forms With Erasures, Alterations and Tampering Will Not Be Accepted/ProcessedDokument2 SeitenApplication Forms With Erasures, Alterations and Tampering Will Not Be Accepted/ProcessedMiw CortesNoch keine Bewertungen
- App-Form For FacultyDokument5 SeitenApp-Form For FacultyMuhammad Mushtaq AliNoch keine Bewertungen
- University of Wah Application FormDokument7 SeitenUniversity of Wah Application FormHasan Qayyum ChohanNoch keine Bewertungen
- Infectious APDokument7 SeitenInfectious APNick ANoch keine Bewertungen
- Application Form For Admission To M.B.B.S./B.D.S. Faculty of MedicineDokument3 SeitenApplication Form For Admission To M.B.B.S./B.D.S. Faculty of MedicineHarsh SinghNoch keine Bewertungen
- Application For The Post of TGT (English) and TGT (Social Science)Dokument4 SeitenApplication For The Post of TGT (English) and TGT (Social Science)Palhari KumarNoch keine Bewertungen
- University of Sindh: Directorate of Research and Graduate StudiesDokument2 SeitenUniversity of Sindh: Directorate of Research and Graduate StudiesShehzad KhanNoch keine Bewertungen
- SBTP Job Application For SBT 2Dokument2 SeitenSBTP Job Application For SBT 2DildarKhanNoch keine Bewertungen
- Application Form For Orientation CourseDokument3 SeitenApplication Form For Orientation CourseAmit Kurmar SharmaNoch keine Bewertungen
- Application Form For Graduate Program Admission: Jimma UniversityDokument7 SeitenApplication Form For Graduate Program Admission: Jimma UniversityDani TarikuNoch keine Bewertungen
- University of Sargodha: Admission Form For Pharm-D (5 Years Course) (Annual System)Dokument5 SeitenUniversity of Sargodha: Admission Form For Pharm-D (5 Years Course) (Annual System)intzar aliNoch keine Bewertungen
- JOB APPLICATION FORM For BS 1 To BS 16Dokument3 SeitenJOB APPLICATION FORM For BS 1 To BS 16Momina SaadNoch keine Bewertungen
- Kas Secondary Bursary FormDokument4 SeitenKas Secondary Bursary FormSam RuhiNoch keine Bewertungen
- IELTSDokument2 SeitenIELTSedifyNoch keine Bewertungen
- Duplicate Triplicate Certificate Diploma FormDokument2 SeitenDuplicate Triplicate Certificate Diploma FormNew StromeNoch keine Bewertungen
- AdvtDokument5 SeitenAdvtMohd KazimNoch keine Bewertungen
- Notification CCRUM Various Vacancy PostsDokument5 SeitenNotification CCRUM Various Vacancy PostsRajkumarNoch keine Bewertungen
- G.M. LAW COLLEGE, PURI-752003, OdishaDokument4 SeitenG.M. LAW COLLEGE, PURI-752003, OdishaGosend GiftNoch keine Bewertungen
- University of Mumbai: Admission FormDokument4 SeitenUniversity of Mumbai: Admission FormMohaseen Khan S LNoch keine Bewertungen
- Instructions For MBBS Admissions For 2014-2015Dokument17 SeitenInstructions For MBBS Admissions For 2014-2015Avinash GowdaNoch keine Bewertungen
- 505 1 Medical Officer 2017Dokument5 Seiten505 1 Medical Officer 2017Vivek SinghNoch keine Bewertungen
- Form 1: Department of Science and Technology Science Education InstituteDokument7 SeitenForm 1: Department of Science and Technology Science Education InstituteCharizz SahagunNoch keine Bewertungen
- Annexures: Annexure - IDokument35 SeitenAnnexures: Annexure - IAarav DhingraNoch keine Bewertungen
- Application For Membership / Upgrading of MembershipDokument4 SeitenApplication For Membership / Upgrading of MembershipSupun SandanayakaNoch keine Bewertungen
- Admission Form Professional Institute of Medical Science Peshawar, Khyber PakhtunkhwaDokument1 SeiteAdmission Form Professional Institute of Medical Science Peshawar, Khyber Pakhtunkhwasaeedullah afridiNoch keine Bewertungen
- Application Form 2020-21 Part-A: Fellowship in General Infectious DiseasesDokument7 SeitenApplication Form 2020-21 Part-A: Fellowship in General Infectious DiseasesPrashant PalNoch keine Bewertungen
- UoB M.A - M.SC Form (Private Students)Dokument7 SeitenUoB M.A - M.SC Form (Private Students)Homer BalochNoch keine Bewertungen
- Application Form BKT WalujDokument4 SeitenApplication Form BKT WalujMy AllNoch keine Bewertungen
- Application Form RVMP, Rahg, RVMS, RVMF 2018Dokument4 SeitenApplication Form RVMP, Rahg, RVMS, RVMF 2018Azhar HussainNoch keine Bewertungen
- CDF Bursary Form-Colleges & University - RariedaDokument4 SeitenCDF Bursary Form-Colleges & University - Rariedahuduma kisumuNoch keine Bewertungen
- Scholar SchemeDokument5 SeitenScholar SchemeShravan ReddyNoch keine Bewertungen
- Directorate of Higher & Technical Education Application FormDokument3 SeitenDirectorate of Higher & Technical Education Application FormTangha Muklom KunchaNoch keine Bewertungen
- 02 ScholarshipDokument3 Seiten02 ScholarshipSaeed Ali ShahaniNoch keine Bewertungen
- Application Forms and Guidelines For Applicants - VKSPV-Teachers' Interview - 2020-21Dokument6 SeitenApplication Forms and Guidelines For Applicants - VKSPV-Teachers' Interview - 2020-21Vivekananda Kendra80% (5)
- FormsMDMS 2010Dokument12 SeitenFormsMDMS 2010Anant BrarNoch keine Bewertungen
- Punjab Tianjin University of Technology (PTUT), Lahore, PakistanDokument3 SeitenPunjab Tianjin University of Technology (PTUT), Lahore, PakistanM Umer Farooq MughalNoch keine Bewertungen
- Entry Form FresherDokument1 SeiteEntry Form FresherAshirwad BanerjeeNoch keine Bewertungen
- City Planning Ms UniversityDokument5 SeitenCity Planning Ms Universitykrunal1513366Noch keine Bewertungen
- STCW ApplicationDokument2 SeitenSTCW ApplicationSamarendu TiwariNoch keine Bewertungen
- LLB Part IIDokument4 SeitenLLB Part IINaul NbnNoch keine Bewertungen
- University of Engineering and Technology Taxila: Application Form For Hostel Allotment 2018-19Dokument1 SeiteUniversity of Engineering and Technology Taxila: Application Form For Hostel Allotment 2018-19Chaudary Hassan AliNoch keine Bewertungen
- Application Form Check ListDokument3 SeitenApplication Form Check ListWaqar AhmedNoch keine Bewertungen
- Indian Institute of Science Education and Research (Iiser) ThiruvananthapuramDokument5 SeitenIndian Institute of Science Education and Research (Iiser) ThiruvananthapuramAsmaNoch keine Bewertungen
- Masters 2Dokument2 SeitenMasters 2Firoj KhanNoch keine Bewertungen
- Format HPCL Scholarship FormDokument2 SeitenFormat HPCL Scholarship FormthanmayashrijaNoch keine Bewertungen
- Mirpur University of Science & Technology (MUST), Mirpur: Section ADokument5 SeitenMirpur University of Science & Technology (MUST), Mirpur: Section AIshaq SadiqNoch keine Bewertungen
- I. Personal Information: Department of Science and Technology Science Education Institute Bicutan, Taguig CityDokument7 SeitenI. Personal Information: Department of Science and Technology Science Education Institute Bicutan, Taguig CityKhera DonaireNoch keine Bewertungen
- IMA FormDokument3 SeitenIMA FormSandeep OdelaNoch keine Bewertungen
- Exam Form - IIPS-Rev.02Dokument2 SeitenExam Form - IIPS-Rev.02Mohammed ZameerNoch keine Bewertungen
- Amu HRDCDokument11 SeitenAmu HRDCrimiguptaNoch keine Bewertungen
- Mohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormDokument2 SeitenMohi-ud-Din Islamic Medical College Sector D-4, Mirpur (AJ&K) Application FormUsama TariqNoch keine Bewertungen
- RIE Ajmer BEd Med Application FormDokument3 SeitenRIE Ajmer BEd Med Application FormAnweshaBoseNoch keine Bewertungen
- PHD 3 Full Time Appl Format Online 20ResearchCent (1) 1 PDFDokument18 SeitenPHD 3 Full Time Appl Format Online 20ResearchCent (1) 1 PDFMega rani RNoch keine Bewertungen
- Indian Provisional Permanent RegistrationDokument8 SeitenIndian Provisional Permanent RegistrationUdhayashankar DhayalanNoch keine Bewertungen
- Clerk (Income Maintenance): Passbooks Study GuideVon EverandClerk (Income Maintenance): Passbooks Study GuideNoch keine Bewertungen
- Tender DocumentDokument38 SeitenTender DocumentRahim BuxNoch keine Bewertungen
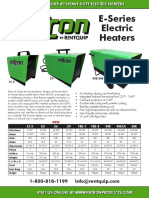
- E-Series Electric Heaters: E1.5 E9 40E/60EDokument2 SeitenE-Series Electric Heaters: E1.5 E9 40E/60ERahim BuxNoch keine Bewertungen
- Self-Contained Drinking Water Cooler: Product Manual ForDokument5 SeitenSelf-Contained Drinking Water Cooler: Product Manual ForRahim BuxNoch keine Bewertungen
- England P3Dokument29 SeitenEngland P3Rahim BuxNoch keine Bewertungen
- The RCD Handbook - Guide To The Selection and Application of Residual Current DevicesDokument42 SeitenThe RCD Handbook - Guide To The Selection and Application of Residual Current DevicesRahim Bux100% (1)
- Someusefulwebsi T Esfortext BooksDokument1 SeiteSomeusefulwebsi T Esfortext BooksRahim BuxNoch keine Bewertungen
- Inspiron 15 3576 Laptop Service Manual en UsDokument136 SeitenInspiron 15 3576 Laptop Service Manual en UsRahim BuxNoch keine Bewertungen
- Unit 31 Fashion Retailing Issue 2Dokument12 SeitenUnit 31 Fashion Retailing Issue 2M.Maulana Iskandar ZulkarnainNoch keine Bewertungen
- Conveying Story Through OrigamiDokument14 SeitenConveying Story Through OrigamifanaliraxNoch keine Bewertungen
- Principles of Foundation Engineering Si Edition 8th Edition Das Solutions ManualDokument21 SeitenPrinciples of Foundation Engineering Si Edition 8th Edition Das Solutions Manualallisontaylorfnrqzamgks100% (23)
- Top Universities in AUstraliaDokument3 SeitenTop Universities in AUstraliaMostofa Khan RohanNoch keine Bewertungen
- Portraits RubricDokument1 SeitePortraits Rubricapi-208041294Noch keine Bewertungen
- ASVAB Math Knowledge Practice Test 4Dokument5 SeitenASVAB Math Knowledge Practice Test 4ASVABTestBankNoch keine Bewertungen
- Acr On Womens Month2023Dokument6 SeitenAcr On Womens Month2023Michelle SedaNoch keine Bewertungen
- Plan of InvestigationDokument9 SeitenPlan of InvestigationAttie's WorldNoch keine Bewertungen
- Cscart Installation LocalDokument12 SeitenCscart Installation LocalMaaz KhanNoch keine Bewertungen
- Dictation in Classroom Tool To Improve ProficiencyDokument10 SeitenDictation in Classroom Tool To Improve Proficiencyandychiak3086Noch keine Bewertungen
- Hyderabad Educators Form - 1 (Responses) - Sheet9Dokument9 SeitenHyderabad Educators Form - 1 (Responses) - Sheet9aruna.sharawatNoch keine Bewertungen
- 50 Habits of Highly Successful PeopleDokument1 Seite50 Habits of Highly Successful Peoplell_pabilonaNoch keine Bewertungen
- Saifullah Ansari-Resume1Dokument1 SeiteSaifullah Ansari-Resume1Saif AnsariNoch keine Bewertungen
- Nursing Diagnosis Need8989Dokument13 SeitenNursing Diagnosis Need8989Banaag JayNoch keine Bewertungen
- Unit 6-Emotion Lesson 1 - Feeling Stressed Look at The Photos A-F. What Emotions Do You Think These People Are Feeling? Why Are They Feeling Them?Dokument4 SeitenUnit 6-Emotion Lesson 1 - Feeling Stressed Look at The Photos A-F. What Emotions Do You Think These People Are Feeling? Why Are They Feeling Them?JoshuaNoch keine Bewertungen
- 51 University of The East vs. JaderDokument3 Seiten51 University of The East vs. JaderGlomarie GonayonNoch keine Bewertungen
- CV Raman PDF Chandrasekhara Venkata RamanDokument2 SeitenCV Raman PDF Chandrasekhara Venkata RamanUUUNoch keine Bewertungen
- About Me Idea Jeric Mar PatocDokument1 SeiteAbout Me Idea Jeric Mar PatocmarsorakunNoch keine Bewertungen
- Assignment ON Intensive and Extensive Reading Activities: Submitted By, S.V. Allan Sharmila, REG. NO: 19BDEN04Dokument7 SeitenAssignment ON Intensive and Extensive Reading Activities: Submitted By, S.V. Allan Sharmila, REG. NO: 19BDEN04AntoNoch keine Bewertungen
- Pluricentric Languages Differing Norms in Different Nations 1nbsped 3110128551 9783110128550Dokument488 SeitenPluricentric Languages Differing Norms in Different Nations 1nbsped 3110128551 9783110128550Bruno CerqueiraNoch keine Bewertungen
- SSC CPO Results 2017 Tier I - FemalesDokument57 SeitenSSC CPO Results 2017 Tier I - FemalesTushitaNoch keine Bewertungen
- Molluscanfamilyp 00 BakeDokument578 SeitenMolluscanfamilyp 00 BakeLi Leny100% (1)
- Upskillnexus PDFDokument8 SeitenUpskillnexus PDFaryankori3635Noch keine Bewertungen
- Configu 5500 GDokument32 SeitenConfigu 5500 GVíctor Humberto Ramírez ParradoNoch keine Bewertungen
- K To 12 Food (Fish) ProcessingDokument20 SeitenK To 12 Food (Fish) Processingjagelido83% (23)
- CIOFF® Festivals Calendar 2014Dokument136 SeitenCIOFF® Festivals Calendar 2014eurodesk.ruralNoch keine Bewertungen
- Comptia Comprehencive Approach 220 901 220 902Dokument834 SeitenComptia Comprehencive Approach 220 901 220 902Sofia LjubicicNoch keine Bewertungen
- Certificate of Community Service: Mary Ann Janeth AmboDokument46 SeitenCertificate of Community Service: Mary Ann Janeth Amboucnursingcesdev2008Noch keine Bewertungen
- DLL - Mapeh 6 - Q3 - W10Dokument3 SeitenDLL - Mapeh 6 - Q3 - W10Yani De Silva100% (1)
- Yumasoft Software SolutionsDokument8 SeitenYumasoft Software SolutionsYumasoftNoch keine Bewertungen