Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Child Nutrition and CookingDokument1 SeiteChild Nutrition and CookingRaysonChooNoch keine Bewertungen
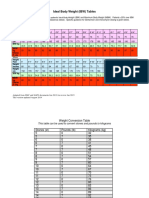
- IBW TableDokument2 SeitenIBW TablegrafikeyesNoch keine Bewertungen
- Libro VM Obeso 2018 PDFDokument305 SeitenLibro VM Obeso 2018 PDFNataly Osorio MarínNoch keine Bewertungen
- I. Physical Fitness TESTING Learning ObjectivesDokument12 SeitenI. Physical Fitness TESTING Learning ObjectivesElain RagosNoch keine Bewertungen
- Introduction To The Banting DietDokument2 SeitenIntroduction To The Banting Dietanisah60Noch keine Bewertungen
- Daftar PustakaDokument5 SeitenDaftar PustakaHanny YulizarNoch keine Bewertungen
- Smart Ketosis Weight Loss On Auto Pilot by Ken Roberts FREE Keto E-BookDokument13 SeitenSmart Ketosis Weight Loss On Auto Pilot by Ken Roberts FREE Keto E-BookKhalilahmad KhatriNoch keine Bewertungen
- Pre-Test Post Test: Health-Related Fitness Health-Related FitnessDokument7 SeitenPre-Test Post Test: Health-Related Fitness Health-Related FitnessArnel BagalawisNoch keine Bewertungen
- Body Fat CalculatorDokument1 SeiteBody Fat CalculatorTom TambeNoch keine Bewertungen
- (PPT) DPC 1.4.1 Periodic Health Examination - Dr. ZuluetaDokument28 Seiten(PPT) DPC 1.4.1 Periodic Health Examination - Dr. ZuluetaJennifer Pisco LiracNoch keine Bewertungen
- Calreqtips PDFDokument2 SeitenCalreqtips PDFP.v.KumarNoch keine Bewertungen
- PH201x IntroductionDokument95 SeitenPH201x IntroductionNur SolichahNoch keine Bewertungen
- Chart WHO + IDAIDokument46 SeitenChart WHO + IDAILovely PoppyNoch keine Bewertungen
- Omega 3 Supplementation Effects On Polycystic Ovary Syndrome Symptoms and Metabolic SyndromeDokument6 SeitenOmega 3 Supplementation Effects On Polycystic Ovary Syndrome Symptoms and Metabolic SyndromerantaikarbonNoch keine Bewertungen
- Royal BCSDokument1 SeiteRoyal BCSIzdaharra Mutia UlfahNoch keine Bewertungen
- Obesity: Pathophysiology and ManagementDokument16 SeitenObesity: Pathophysiology and ManagementNurulAzizahAnNoch keine Bewertungen
- 2016 European Guidelines On Cardiovascular Disease Prevention in Clinical PracticeDokument78 Seiten2016 European Guidelines On Cardiovascular Disease Prevention in Clinical PracticeJose Ignacio Tarton SisimitNoch keine Bewertungen
- Problem Solution Essay: How-Tos!Dokument40 SeitenProblem Solution Essay: How-Tos!Khánh Ly NguyễnNoch keine Bewertungen
- FAandDZ PDFDokument8 SeitenFAandDZ PDFCosmin GabrielNoch keine Bewertungen
- Open Letter To Diet CultureDokument3 SeitenOpen Letter To Diet Cultureapi-495190351Noch keine Bewertungen
- Diabetes Clinical Practice Recommendations, ADA2008 PDFDokument104 SeitenDiabetes Clinical Practice Recommendations, ADA2008 PDFUchy CutejhyNoch keine Bewertungen
- CHAPTER 1-pathfit1-REACTION PAPERDokument6 SeitenCHAPTER 1-pathfit1-REACTION PAPERMark ChristianNoch keine Bewertungen
- Exercises Class November 10thDokument5 SeitenExercises Class November 10thagatinha01.laraNoch keine Bewertungen
- For More Books and Articles Join To The Channel in Telegram: Published By/ D.T Mahmoud SultanDokument4 SeitenFor More Books and Articles Join To The Channel in Telegram: Published By/ D.T Mahmoud SultanNeama MNoch keine Bewertungen
- Obesity Reading ComprehensionDokument3 SeitenObesity Reading ComprehensionDaniela SarmientoNoch keine Bewertungen
- Parental Knowledge and Perception of Childhood Obesity-Review ModelDokument14 SeitenParental Knowledge and Perception of Childhood Obesity-Review ModelSENGOTTUVEL CHENNIAPPANNoch keine Bewertungen
- Eating and Exercise Activity NotesDokument3 SeitenEating and Exercise Activity Noteswalter jesusNoch keine Bewertungen
- Unit 2: Active Recreation (Fitness)Dokument9 SeitenUnit 2: Active Recreation (Fitness)Aj AntonioNoch keine Bewertungen
- 0 IELTS Writing Test - Complex SentencesDokument12 Seiten0 IELTS Writing Test - Complex SentencesCataA.GestaNoch keine Bewertungen
- Focusing On Language Pproprojectlanguage: My Family and NeighborsDokument3 SeitenFocusing On Language Pproprojectlanguage: My Family and NeighborsYanella Vega FloresNoch keine Bewertungen