Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Case AclDokument15 SeitenCase AclRashi JainNoch keine Bewertungen
- Biomechanics of Patellofemoral Joint': Ronald P. Grelsamer, MD" John R. Klein, MDDokument13 SeitenBiomechanics of Patellofemoral Joint': Ronald P. Grelsamer, MD" John R. Klein, MDBrunoNoch keine Bewertungen
- How To Squat - The Definitive Guide - Stronger by ScienceDokument95 SeitenHow To Squat - The Definitive Guide - Stronger by ScienceNilgunNoch keine Bewertungen
- Anatomy (Patellofemoral Joint)Dokument3 SeitenAnatomy (Patellofemoral Joint)Andy Delos ReyesNoch keine Bewertungen
- SCR Sept 2017 PDF-1Dokument61 SeitenSCR Sept 2017 PDF-1Manuel PomboNoch keine Bewertungen
- 7 Exercises in 7 Minutes To Never Feel Lower Back Pain AgainDokument6 Seiten7 Exercises in 7 Minutes To Never Feel Lower Back Pain AgainDexter Precioso100% (1)
- Supple Leopard Mobility NotesDokument4 SeitenSupple Leopard Mobility Notesbtwx67% (3)
- My Workout Plan - Ulysses Ramirez Hed 44Dokument3 SeitenMy Workout Plan - Ulysses Ramirez Hed 44api-357635895Noch keine Bewertungen
- Girevoy Sport and Athlete PreparationDokument90 SeitenGirevoy Sport and Athlete Preparationpieguy314Noch keine Bewertungen
- Training To Pickup WomenDokument12 SeitenTraining To Pickup WomenMilica PopovicNoch keine Bewertungen
- Orthopedic Chart 3-3Dokument9 SeitenOrthopedic Chart 3-3elaine daiNoch keine Bewertungen
- Effect of Patellar Taping On Knee Kinetics of Patients With Patellofemoral Pain SyndromeDokument7 SeitenEffect of Patellar Taping On Knee Kinetics of Patients With Patellofemoral Pain SyndromeRuben CapelaNoch keine Bewertungen
- 400w43 e Poster Gangphasen Druck PDFDokument1 Seite400w43 e Poster Gangphasen Druck PDFDejan Milenkovic50% (2)
- Iron Man - USA 1 2006Dokument165 SeitenIron Man - USA 1 2006api-6141969467% (3)
- Nobull 23Dokument35 SeitenNobull 23B D Cook100% (2)
- Analysis-Female Body BreakthroughDokument92 SeitenAnalysis-Female Body BreakthroughAntonio HenryNoch keine Bewertungen
- TKR ProtocolDokument8 SeitenTKR ProtocolSandeep SoniNoch keine Bewertungen
- Muscle Science RoundupDokument165 SeitenMuscle Science RoundupAlessandro Valentim100% (2)
- Self Massage Therapy Guide - Physix Gear Sport PDFDokument25 SeitenSelf Massage Therapy Guide - Physix Gear Sport PDFAlexandria Trahan100% (1)
- Injury Prevention Exercises For RunnersDokument12 SeitenInjury Prevention Exercises For RunnerselianaecheverrymNoch keine Bewertungen
- Rehabilitation: Walking After Total Knee ReplacementDokument10 SeitenRehabilitation: Walking After Total Knee ReplacementSandeep DhimanNoch keine Bewertungen
- Schellenberg Et Al., 2017 Towards Evidence Based Strength Training A Compatison of Muscle Forces During Deadlifts, Goodmornings and Split SquatsDokument10 SeitenSchellenberg Et Al., 2017 Towards Evidence Based Strength Training A Compatison of Muscle Forces During Deadlifts, Goodmornings and Split SquatsDebora CantergiNoch keine Bewertungen
- Vertical Jump Handbook Ver. 1.0 - Shot Science BasketballDokument31 SeitenVertical Jump Handbook Ver. 1.0 - Shot Science Basketball송필용Noch keine Bewertungen
- Muscular SystemDokument1 SeiteMuscular SystemChris_Barber09100% (1)
- A Brief Review On The Effects of The Squat Exercise On Lower Limb Muscle HypertrophyDokument10 SeitenA Brief Review On The Effects of The Squat Exercise On Lower Limb Muscle HypertrophyDaniel FreireNoch keine Bewertungen
- Chondro Malacia PatellaDokument16 SeitenChondro Malacia Patellamedical- physio classesNoch keine Bewertungen
- Beating Patellar Tendonitis Exercise Pictures PDFDokument16 SeitenBeating Patellar Tendonitis Exercise Pictures PDFNoel Martin100% (1)
- Quad Destroyer - 10 Sets of Squats Workout - Muscle & StrengthDokument6 SeitenQuad Destroyer - 10 Sets of Squats Workout - Muscle & StrengthMouhNoch keine Bewertungen
- Yoga Therapy For Your KneesDokument8 SeitenYoga Therapy For Your KneesHendrik Gurbaxingh de MeidaiNoch keine Bewertungen
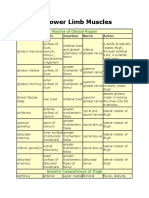
- Lower Limb MusclesDokument8 SeitenLower Limb Musclesbilal_kmu020% (1)