Das könnte Ihnen auch gefallen
- Periodontics: Treatment Planning For Patients With Periodontal DiseasesDokument17 SeitenPeriodontics: Treatment Planning For Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNoch keine Bewertungen
- Problem in Complete Denture Treatment and Postinsertion DentureDokument35 SeitenProblem in Complete Denture Treatment and Postinsertion DentureSorabh JainNoch keine Bewertungen
- 1 s2.0 S001185322200595X MainDokument15 Seiten1 s2.0 S001185322200595X MainRashmita NayakNoch keine Bewertungen
- Maintainence Phase of Periodontal CareDokument4 SeitenMaintainence Phase of Periodontal CareDeen MohdNoch keine Bewertungen
- The Treatment Plan: Dr. Omar SolimanDokument36 SeitenThe Treatment Plan: Dr. Omar SolimanSamwel EmadNoch keine Bewertungen
- Prostho KLP 9 EtaDokument3 SeitenProstho KLP 9 EtaAinul MardiahNoch keine Bewertungen
- Perio Paper-FinalDokument8 SeitenPerio Paper-Finalapi-547158281Noch keine Bewertungen
- Chao Pinhole Surgical Technique Consent FormDokument2 SeitenChao Pinhole Surgical Technique Consent FormDavidNoch keine Bewertungen
- Periodontics: Dentistry DepartmentDokument10 SeitenPeriodontics: Dentistry DepartmentmahmoodNoch keine Bewertungen
- Periodontal Maintenance - A ReviewDokument7 SeitenPeriodontal Maintenance - A ReviewVanessa MordiNoch keine Bewertungen
- Dental AidDokument6 SeitenDental AidCroitort530% (1)
- CD CareDokument8 SeitenCD CareAkshayNoch keine Bewertungen
- Perio EssayDokument7 SeitenPerio Essayapi-252614255Noch keine Bewertungen
- SDCEP Periodontal Disease Guidance in BriefDokument19 SeitenSDCEP Periodontal Disease Guidance in BriefLupu AndreeaNoch keine Bewertungen
- Nebdn National Diploma in Dental Nursing Practical Experience Record SheetDokument8 SeitenNebdn National Diploma in Dental Nursing Practical Experience Record SheetCamila Walton100% (6)
- Kkamm Perio Research PaperDokument8 SeitenKkamm Perio Research Paperapi-455560394Noch keine Bewertungen
- Reflection - Patient EvalDokument1 SeiteReflection - Patient Evalapi-733563770Noch keine Bewertungen
- FCD Ethical and Legal IssuesDokument6 SeitenFCD Ethical and Legal Issuesnicholas51292Noch keine Bewertungen
- E PerioTherapyDokument5 SeitenE PerioTherapyFerdinan PasaribuNoch keine Bewertungen
- Phase I TherapyDokument11 SeitenPhase I TherapygopzzzzNoch keine Bewertungen
- Perio Paper 1Dokument9 SeitenPerio Paper 1api-733563770Noch keine Bewertungen
- Periodontal Therapy StatementDokument7 SeitenPeriodontal Therapy StatementDiana AlexandraNoch keine Bewertungen
- Periodontal Research PaperDokument8 SeitenPeriodontal Research Paperapi-279944111Noch keine Bewertungen
- Prevent MeasuresDokument1 SeitePrevent Measuresapi-742616973Noch keine Bewertungen
- Presentation 1. Treatment Planning For The Immediate Denture 2. The Patient With Periodontal DiseaseDokument19 SeitenPresentation 1. Treatment Planning For The Immediate Denture 2. The Patient With Periodontal DiseaseNika Permata DelaNoch keine Bewertungen
- Pag 67Dokument1 SeitePag 67Arjun NarangNoch keine Bewertungen
- Diagnosis and Treatment Planning For Partially Edentulous Patients11Dokument160 SeitenDiagnosis and Treatment Planning For Partially Edentulous Patients11Rajsandeep Singh80% (5)
- Failures in Periodontal Therapy: Review ArticleDokument6 SeitenFailures in Periodontal Therapy: Review ArticlezinniaNoch keine Bewertungen
- Supportive Periodontal TherapyDokument58 SeitenSupportive Periodontal TherapyPriyanka TripathiNoch keine Bewertungen
- Prosthodontics Lec 2 PDFDokument25 SeitenProsthodontics Lec 2 PDFHassan QazaniNoch keine Bewertungen
- 7 LecturesDokument11 Seiten7 Lecturesعبد المجيد المصلحNoch keine Bewertungen
- Diabetes Prostho ManagementDokument5 SeitenDiabetes Prostho ManagementneethuNoch keine Bewertungen
- Treatment PlanDokument21 SeitenTreatment PlanRajani Gedela0% (1)
- D L, H R & L L: Periodontology 2000Dokument24 SeitenD L, H R & L L: Periodontology 2000ph4nt0mgr100% (1)
- Management of Oral Cancer (1) ...Dokument3 SeitenManagement of Oral Cancer (1) ...Mircea IlieNoch keine Bewertungen
- RISMINDokument18 SeitenRISMINVerghese JobNoch keine Bewertungen
- The Management of Gingival Hyperplasia On Patient With Orthodontic TreatmentDokument7 SeitenThe Management of Gingival Hyperplasia On Patient With Orthodontic TreatmentPuspandaru Nur Iman FadlilNoch keine Bewertungen
- Short AnswersDokument41 SeitenShort AnswersChander KantaNoch keine Bewertungen
- Patient CareDokument3 SeitenPatient CareAistė AgapovaitėNoch keine Bewertungen
- Complete Yourself: Fixed Teeth in One Day With The All-On-4 Treatment ConceptDokument16 SeitenComplete Yourself: Fixed Teeth in One Day With The All-On-4 Treatment ConceptNaunit VaidNoch keine Bewertungen
- Diagnosis and Treatment Planning - Removable Partial Denture Part-1Dokument38 SeitenDiagnosis and Treatment Planning - Removable Partial Denture Part-1Ahmed AliNoch keine Bewertungen
- Adjuncts To Mouth Reconstruction S.: Alexander Forster, New York, N. YDokument5 SeitenAdjuncts To Mouth Reconstruction S.: Alexander Forster, New York, N. YAmar BhochhibhoyaNoch keine Bewertungen
- Preventive ProsthodonticsDokument13 SeitenPreventive Prosthodonticsbhuvanesh4668100% (1)
- ODTP - 4 Tooth Surface LossDokument7 SeitenODTP - 4 Tooth Surface LossDr-Mohamed KandeelNoch keine Bewertungen
- Palliative Dental 2014Dokument6 SeitenPalliative Dental 2014Isteicy CortezNoch keine Bewertungen
- Detailed Case History in C - DDokument54 SeitenDetailed Case History in C - Dvahini niharika100% (8)
- Post Insertion InstructionsDokument23 SeitenPost Insertion InstructionsAnkita Reddy VallapNoch keine Bewertungen
- Periodontal Considerations in RPDDokument69 SeitenPeriodontal Considerations in RPDPuneet Pandher100% (2)
- Introduction To Preventive DentistryDokument4 SeitenIntroduction To Preventive DentistryHaider F YehyaNoch keine Bewertungen
- Oral Diagnosis and Treatment Planning: Part 8. Reviews and Maintenance of RestorationsDokument8 SeitenOral Diagnosis and Treatment Planning: Part 8. Reviews and Maintenance of RestorationsBibek RajNoch keine Bewertungen
- Oral Health ProgramDokument8 SeitenOral Health Programapi-292263050Noch keine Bewertungen
- Ce 50Dokument20 SeitenCe 50Debbie OngNoch keine Bewertungen
- SAQs VariousDokument16 SeitenSAQs Variousapi-26291651100% (3)
- Nursing Management of Oral HygieneDokument40 SeitenNursing Management of Oral HygieneMheanne RomanoNoch keine Bewertungen
- A. Medical Review: B. Affective Sociological and Psychological Review. C. Dental HistoryDokument6 SeitenA. Medical Review: B. Affective Sociological and Psychological Review. C. Dental HistoryHayder MaqsadNoch keine Bewertungen
- Ailments RemediesDokument219 SeitenAilments RemediesSubramanya RaoNoch keine Bewertungen
- Prenatal Care Case PresentationDokument32 SeitenPrenatal Care Case PresentationMary Grace Mas100% (1)
- Suvarna H PatilDokument7 SeitenSuvarna H Patildaniel_siitompulNoch keine Bewertungen
- Prostho IV - Slide 3 - Impression - Making - For - Complete - DenturesDokument82 SeitenProstho IV - Slide 3 - Impression - Making - For - Complete - Denturesبراءة أحمد السلامات100% (1)
- Adel Lecture 3Dokument6 SeitenAdel Lecture 3jesuscomingsoon2005_Noch keine Bewertungen
- Periodontal Plastic and Esthetic Surgery.Dokument86 SeitenPeriodontal Plastic and Esthetic Surgery.Mohammed Ahmed TawfikNoch keine Bewertungen
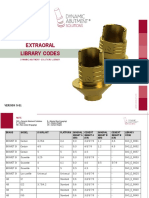
- Extraoral Library Codes: VERSION 5-81Dokument26 SeitenExtraoral Library Codes: VERSION 5-81Zsolt PerényiNoch keine Bewertungen
- ICD-10 Dental Diagnosis CodesDokument7 SeitenICD-10 Dental Diagnosis CodesGenevieve Florencia Natasya SaraswatiNoch keine Bewertungen
- Rick 2004 OmscnaDokument22 SeitenRick 2004 OmscnakiwibolNoch keine Bewertungen
- Removable PARTIAL DENTURE THEORY AND PRACTICEDokument643 SeitenRemovable PARTIAL DENTURE THEORY AND PRACTICEMostafa Fayad94% (16)
- Frenectomy and FrenotomyDokument24 SeitenFrenectomy and Frenotomymathurarun2000Noch keine Bewertungen
- Oral Submucous FibrosisDokument59 SeitenOral Submucous Fibrosisvishalzenia100% (3)
- Lingual Orthodontics PDFDokument202 SeitenLingual Orthodontics PDFYan-HongLin100% (1)
- Optimizing Gingival EstheticsDokument8 SeitenOptimizing Gingival EstheticsThe Bioclear Clinic100% (1)
- Immediate DentureDokument48 SeitenImmediate DenturesunithabanavathNoch keine Bewertungen
- Removable Partial DentureDokument3 SeitenRemovable Partial DentureKim Philip YuntingNoch keine Bewertungen
- #2 PEDO - Dental Charting & NotationDokument24 Seiten#2 PEDO - Dental Charting & NotationomeerulrafieNoch keine Bewertungen
- Dento Alveolar FracturesDokument16 SeitenDento Alveolar FracturesafifrspmNoch keine Bewertungen
- A Clinical Overview of Removable Prostheses 3. Principles of Design For Removable Partial DenturesDokument7 SeitenA Clinical Overview of Removable Prostheses 3. Principles of Design For Removable Partial DenturesMohsin HabibNoch keine Bewertungen
- SipDokument12 SeitenSipadi3636Noch keine Bewertungen
- Mandibular Major ConnectorsDokument47 SeitenMandibular Major ConnectorsdghnairNoch keine Bewertungen
- Gingival RetractionDokument18 SeitenGingival RetractionSonam RastogiNoch keine Bewertungen
- Periapical SurgeryDokument107 SeitenPeriapical SurgeryShaliniNoch keine Bewertungen
- اسئلة الهيئة لطب الاسنانDokument65 Seitenاسئلة الهيئة لطب الاسنانSara El HadidiNoch keine Bewertungen
- Characteristics and Uses of CollagenDokument6 SeitenCharacteristics and Uses of CollagenRoxana ElenaNoch keine Bewertungen
- Class IV RestorasiDokument6 SeitenClass IV RestorasiNovi YantiNoch keine Bewertungen
- Farnoush 1978Dokument3 SeitenFarnoush 1978Kyoko CPNoch keine Bewertungen
- Periodontitis and Systemic DiseasesDokument55 SeitenPeriodontitis and Systemic DiseasesDr.Arshad SayedNoch keine Bewertungen
- Complications and Failures of ImplantsDokument35 SeitenComplications and Failures of ImplantssavNoch keine Bewertungen
- Patient Information For InvisalignDokument10 SeitenPatient Information For InvisalignHarry ArdiyantoNoch keine Bewertungen