Das könnte Ihnen auch gefallen
- Policies and Procedures Manual TemplateDokument220 SeitenPolicies and Procedures Manual Templatedoctorlupu100% (3)
- Protocol Clinic Proteze BPS IvoclarDokument38 SeitenProtocol Clinic Proteze BPS IvoclarOvidiu SchifirnetNoch keine Bewertungen
- Mouth Preparation - PDF 161301Dokument127 SeitenMouth Preparation - PDF 161301S ل DentistNoch keine Bewertungen
- PLPF PDFDokument88 SeitenPLPF PDFmaxNoch keine Bewertungen
- First Page PDFDokument1 SeiteFirst Page PDFJordan BzNoch keine Bewertungen
- Understanding Depression and SuicideDokument27 SeitenUnderstanding Depression and Suicideproject creatorNoch keine Bewertungen
- 5 Steps To A Successful Dental PracticeDokument22 Seiten5 Steps To A Successful Dental PracticeVasile FlorinNoch keine Bewertungen
- 2 Anatomy of TMJDokument117 Seiten2 Anatomy of TMJSugandhi Pidaparthi100% (1)
- Principles of Complex Exodontia: Oral Surgery IIDokument45 SeitenPrinciples of Complex Exodontia: Oral Surgery IIRayne GelleNoch keine Bewertungen
- Implant Course.Dokument76 SeitenImplant Course.mustafaNoch keine Bewertungen
- Common Mistakes in Clinical Dental PracticeDokument80 SeitenCommon Mistakes in Clinical Dental PracticeRohit ShahNoch keine Bewertungen
- Vsip - Info - Anterior Wax Up PDF Free PDFDokument3 SeitenVsip - Info - Anterior Wax Up PDF Free PDFMekideche dental officeNoch keine Bewertungen
- COD Comprehensaive Clinic ManualDokument105 SeitenCOD Comprehensaive Clinic ManualdoctorlupuNoch keine Bewertungen
- State of The ArtDokument3 SeitenState of The ArtArne HeyerickNoch keine Bewertungen
- Dentoalveoar SurgeryDokument131 SeitenDentoalveoar SurgeryRujan Mirela AmaliaNoch keine Bewertungen
- Implant Patient Surgery Information and Consent FormDokument5 SeitenImplant Patient Surgery Information and Consent FormtinkfayeNoch keine Bewertungen
- RCDSO Guidelines Implant Dentistry PDFDokument16 SeitenRCDSO Guidelines Implant Dentistry PDFl4j0b9Noch keine Bewertungen
- Marketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanVon EverandMarketing Implant Dentistry: Attract and Influence Patients to Accept Your Dental Implant Treatment PlanNoch keine Bewertungen
- Implant Consent Form1Dokument2 SeitenImplant Consent Form1Jitender ReddyNoch keine Bewertungen
- Osce, BaselDokument302 SeitenOsce, Baselbpjavi78% (9)
- Multimedia PDFDokument16 SeitenMultimedia PDFadamNoch keine Bewertungen
- Introduction of Removable Partial Denture - Design and RetentionDokument72 SeitenIntroduction of Removable Partial Denture - Design and RetentionDilesh Pradhan0% (1)
- Dental OsteologyDokument154 SeitenDental OsteologyfabrizioaryanNoch keine Bewertungen
- Wax Contouring of CD ReportDokument10 SeitenWax Contouring of CD ReportAbdullah Muhammed khaleel HassanNoch keine Bewertungen
- Risk FactorsDokument174 SeitenRisk FactorsdevikaNoch keine Bewertungen
- Pre Treatment Assesment of ImplantDokument19 SeitenPre Treatment Assesment of Implantdrgayen6042Noch keine Bewertungen
- Calcium Silicate-Based Root Canal SealersDokument21 SeitenCalcium Silicate-Based Root Canal SealersdoctorlupuNoch keine Bewertungen
- Dentaltown 2018marchDokument113 SeitenDentaltown 2018marchDanutz BalanNoch keine Bewertungen
- Drug Study of TBDokument7 SeitenDrug Study of TBMarc AntonioNoch keine Bewertungen
- Jurnal BTKV Herman 1Dokument11 SeitenJurnal BTKV Herman 1Elyas MuhammadNoch keine Bewertungen
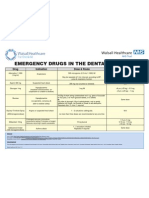
- Emergency Drugs Poster - Layout 1 in Dental PracticeDokument1 SeiteEmergency Drugs Poster - Layout 1 in Dental PracticeFady AtefNoch keine Bewertungen
- Common Breast DiseasesDokument64 SeitenCommon Breast Diseasesamirahmei100% (1)
- Clin DSDDokument5 SeitenClin DSDAlfred OrozcoNoch keine Bewertungen
- Periodontal-Restorative Interactions: A Review: DentistryDokument7 SeitenPeriodontal-Restorative Interactions: A Review: DentistrySahana RangarajanNoch keine Bewertungen
- Evaluation of The Relationship Between Bruxism and Premature Occlusal ContactsDokument6 SeitenEvaluation of The Relationship Between Bruxism and Premature Occlusal ContactsWellyAnggarani100% (1)
- Breastfeeding Tsek AdvocacyDokument81 SeitenBreastfeeding Tsek AdvocacyBelle A. Basilio100% (3)
- Managing The Unstable CDDokument8 SeitenManaging The Unstable CDNajeeb UllahNoch keine Bewertungen
- Perinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornDokument210 SeitenPerinatology Clinics 2008, Vol.35, Issues 4, Neuroprotection in The NewbornJhonny MarquezNoch keine Bewertungen
- Papper PeriodDokument12 SeitenPapper PeriodLoretoReyesMoralesNoch keine Bewertungen
- Fixed Orthodontic Appliances: A Practical GuideVon EverandFixed Orthodontic Appliances: A Practical GuideBewertung: 1 von 5 Sternen1/5 (1)
- Introduction To OcclusionDokument56 SeitenIntroduction To OcclusionSuvasish SuvasishNoch keine Bewertungen
- MGE Case Acceptance Ebook 2018 PDFDokument22 SeitenMGE Case Acceptance Ebook 2018 PDFMavisNoch keine Bewertungen
- ITI Decision Tree Immediate PlacementDokument1 SeiteITI Decision Tree Immediate Placementxiaoxin zhangNoch keine Bewertungen
- Swift Series Clinical Governance Book Edition 1Dokument69 SeitenSwift Series Clinical Governance Book Edition 1Lily Hariri100% (1)
- Optimization of Emergence Profile of Implant ProstDokument8 SeitenOptimization of Emergence Profile of Implant ProstAya Ibrahim YassinNoch keine Bewertungen
- 1 s2.0 S0022391302002998 MainDokument5 Seiten1 s2.0 S0022391302002998 MainManjeev GuragainNoch keine Bewertungen
- Cosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseDokument21 SeitenCosmetic Dentistry & Aesthetic Restorative Dentistry: Comprehensive One-Year CourseMariusNONoch keine Bewertungen
- LiverpoolSedation ManagementDokument9 SeitenLiverpoolSedation ManagementTheresia Avila KurniaNoch keine Bewertungen
- Dental InformaticsDokument43 SeitenDental InformaticsKarim AhmedNoch keine Bewertungen
- A A D W - Up: N Dvanced Iagnostic AxDokument4 SeitenA A D W - Up: N Dvanced Iagnostic AxjoephinNoch keine Bewertungen
- Reducing The Risk of Failure Incomplete Denture PatientsDokument8 SeitenReducing The Risk of Failure Incomplete Denture PatientsHisyam IshakNoch keine Bewertungen
- Impact of Lateral Occlusion Schemes: A Systematic ReviewDokument12 SeitenImpact of Lateral Occlusion Schemes: A Systematic ReviewCristobalVeraNoch keine Bewertungen
- Bicon Seating ChecklistDokument2 SeitenBicon Seating ChecklistRoger VergarayNoch keine Bewertungen
- Erosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Dokument82 SeitenErosion Abrasion Attrition and Abfrcation1Erosion Abrasion Attrition and Abfrcation1Madalina A DobreNoch keine Bewertungen
- Telescopic Dentures: An Overlooked TechnologyDokument3 SeitenTelescopic Dentures: An Overlooked TechnologyarchanglsNoch keine Bewertungen
- Preprosthetic and Reconstructive SurgeryDokument32 SeitenPreprosthetic and Reconstructive Surgeryruoiconmapu100% (1)
- Dentistry: Primary Dental Care Services in England and WalesDokument72 SeitenDentistry: Primary Dental Care Services in England and WalesAyman BafaQeehNoch keine Bewertungen
- Accuracy of Digital Impressions of Multiple Dental Implants An in Vitro StudyDokument6 SeitenAccuracy of Digital Impressions of Multiple Dental Implants An in Vitro StudyFellipeCarvalhoNoch keine Bewertungen
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDokument11 SeitenOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcNoch keine Bewertungen
- Pros FullDokument249 SeitenPros FullAsem Debris100% (1)
- Accurate ALginate ImpressionDokument2 SeitenAccurate ALginate Impressionlah_saneNoch keine Bewertungen
- Volumetric Shrinkage and Film THDokument8 SeitenVolumetric Shrinkage and Film THcalebleon101113Noch keine Bewertungen
- Informed Consent For Crown and Bridge ProstheticsDokument3 SeitenInformed Consent For Crown and Bridge ProstheticsVikkii VeerakumarNoch keine Bewertungen
- Vital Therapy in Carious ToothDokument9 SeitenVital Therapy in Carious ToothAsh PeiNoch keine Bewertungen
- SSCDokument50 SeitenSSCMustafa Tambawala100% (1)
- 2013 Direct Anterior Composites A Practical GuideDokument16 Seiten2013 Direct Anterior Composites A Practical Guidemaroun ghalebNoch keine Bewertungen
- Caries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFDokument7 SeitenCaries Detection and Diagnosis Sealants and Management of The Possibly Carious Fissure PDFGen LCNoch keine Bewertungen
- Chu's Aesthetic Gauge BrochureDokument2 SeitenChu's Aesthetic Gauge BrochureHugoRoCkstarNoch keine Bewertungen
- Biomechanics and Clinical Implications of Complete Edentulous StateDokument4 SeitenBiomechanics and Clinical Implications of Complete Edentulous StateDorobantuMihaiGabiNoch keine Bewertungen
- The Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingDokument13 SeitenThe Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingMikeunoeNoch keine Bewertungen
- Modern Endodontic Principes IrrigationDokument10 SeitenModern Endodontic Principes IrrigationDulgheru StefanNoch keine Bewertungen
- Modern Endodontic Principles Part 2 Access and StrategypdfDokument9 SeitenModern Endodontic Principles Part 2 Access and StrategypdfdoctorlupuNoch keine Bewertungen
- ANATOMIE 23RadixEntomolarispp87 90.20190614125011Dokument4 SeitenANATOMIE 23RadixEntomolarispp87 90.20190614125011doctorlupuNoch keine Bewertungen
- Modern Endodontic Principles Part 7 The Restorative InterfaceDokument12 SeitenModern Endodontic Principles Part 7 The Restorative InterfacedoctorlupuNoch keine Bewertungen
- Modern Endodontic Principles Part 1 Assessing Complexity and Predicting SuccessDokument11 SeitenModern Endodontic Principles Part 1 Assessing Complexity and Predicting SuccessdoctorlupuNoch keine Bewertungen
- Minimally Invasive When? How? Why?: Access Cavity Preparation in EndodonticsDokument4 SeitenMinimally Invasive When? How? Why?: Access Cavity Preparation in EndodonticsdoctorlupuNoch keine Bewertungen
- RCDSO Guidelines Electronic Records ManagementDokument16 SeitenRCDSO Guidelines Electronic Records ManagementdoctorlupuNoch keine Bewertungen
- RCDSO Medical History Recordkeeping GuideDokument13 SeitenRCDSO Medical History Recordkeeping GuidedoctorlupuNoch keine Bewertungen
- Rcdso Ipac Selfaudit FormDokument15 SeitenRcdso Ipac Selfaudit FormdoctorlupuNoch keine Bewertungen
- RCDSO Guidelines Diagnosis and Management of TMDDokument12 SeitenRCDSO Guidelines Diagnosis and Management of TMDdoctorlupuNoch keine Bewertungen
- RCDSO Medical History HandoutDokument1 SeiteRCDSO Medical History HandoutdoctorlupuNoch keine Bewertungen
- RCDSO Guidelines Dental RecordkeepingDokument18 SeitenRCDSO Guidelines Dental RecordkeepingdoctorlupuNoch keine Bewertungen
- RCDSO Guidelines Conflict of InterestDokument4 SeitenRCDSO Guidelines Conflict of InterestdoctorlupuNoch keine Bewertungen
- RCDSO - 4884 Policy Manual v.2Dokument13 SeitenRCDSO - 4884 Policy Manual v.2doctorlupuNoch keine Bewertungen
- The Revised National Tuberculosis Control ProgrammeDokument2 SeitenThe Revised National Tuberculosis Control ProgrammesuryaslideNoch keine Bewertungen
- Bola CommunityDokument5 SeitenBola CommunityOladimeji Raphael OnibonNoch keine Bewertungen
- Topic 3 Environmental Risk AssessmentDokument47 SeitenTopic 3 Environmental Risk Assessment郭思凱Noch keine Bewertungen
- Presc Audit ReportDokument85 SeitenPresc Audit ReportAnuj KaushalNoch keine Bewertungen
- Practice Problems ADokument2 SeitenPractice Problems ACrystal LynaeNoch keine Bewertungen
- DTCO-KURNOOL - Anti TB Day (3rd Friday) Reporting Format - Phc-RegardingDokument8 SeitenDTCO-KURNOOL - Anti TB Day (3rd Friday) Reporting Format - Phc-Regardingkodathalapallis24Noch keine Bewertungen
- MS SDS SR Repo Ort: Name of S Model SampleDokument7 SeitenMS SDS SR Repo Ort: Name of S Model SampleCamilo WispNoch keine Bewertungen
- The British Journal of Cardiology May-June 2010, Volume 17 Supplement 2Dokument16 SeitenThe British Journal of Cardiology May-June 2010, Volume 17 Supplement 2mbarrales_4Noch keine Bewertungen
- Anti TuberDokument16 SeitenAnti TuberpgfhgfgfNoch keine Bewertungen
- Review of Related LiteratureDokument6 SeitenReview of Related Literaturegilrae merlanNoch keine Bewertungen
- Stem12bsn2 Casestudy5 PDFDokument12 SeitenStem12bsn2 Casestudy5 PDFShane TabalbaNoch keine Bewertungen
- Burn Emergency Management For The First Responder-Layout VDokument16 SeitenBurn Emergency Management For The First Responder-Layout VnikitagustiNoch keine Bewertungen
- Copyofresume TraditionalDokument4 SeitenCopyofresume Traditionalapi-282124625Noch keine Bewertungen
- Livedoidna VaskulopatijaDokument5 SeitenLivedoidna VaskulopatijaemirkurtalicNoch keine Bewertungen
- Topical Analgesics: Murilo Pereira Flores, Anita Perpetua Carvalho Rocha de Castro, Jedson Dos Santos NascimentoDokument9 SeitenTopical Analgesics: Murilo Pereira Flores, Anita Perpetua Carvalho Rocha de Castro, Jedson Dos Santos NascimentoYanuar FajarNoch keine Bewertungen
- A Huge Completely Isolated Duplication CystDokument6 SeitenA Huge Completely Isolated Duplication CystNurlyanti RustamNoch keine Bewertungen
- Biology Matters 3rd EditionDokument272 SeitenBiology Matters 3rd Editionotakukat763Noch keine Bewertungen
- Dysbiosis of The Human Oral Microbiome During The Menstrual Cycle and Vulnerability To The External Exposures of Smoking and Dietary SugarDokument14 SeitenDysbiosis of The Human Oral Microbiome During The Menstrual Cycle and Vulnerability To The External Exposures of Smoking and Dietary SugarPaloma C. PeñaNoch keine Bewertungen
- DAFTAR PUSTAKA HydrocephalusDokument2 SeitenDAFTAR PUSTAKA HydrocephalusRahma darisNoch keine Bewertungen
- Elc501 - Group Portfolio ForumDokument11 SeitenElc501 - Group Portfolio ForumAhmad SyamiNoch keine Bewertungen
- One Lung Ventilation: General Principles - UpToDateDokument26 SeitenOne Lung Ventilation: General Principles - UpToDateAna Belén Artero CastañoNoch keine Bewertungen
- Immunofluorescence Techniques: Ian D. Odell and Deborah CookDokument4 SeitenImmunofluorescence Techniques: Ian D. Odell and Deborah CookbalamurugantNoch keine Bewertungen