Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Introduction Biology Humoral and Cell Mediated ResponseDokument3 SeitenIntroduction Biology Humoral and Cell Mediated ResponseReshana SimonNoch keine Bewertungen
- SUBSTANCE ABUSE Biology PresentationDokument12 SeitenSUBSTANCE ABUSE Biology PresentationReshana SimonNoch keine Bewertungen
- Lecture Xiii - Health and DiseaseDokument8 SeitenLecture Xiii - Health and DiseaseJennelle CadoganNoch keine Bewertungen
- Soil pH Management for Optimal Crop YieldsDokument6 SeitenSoil pH Management for Optimal Crop YieldsChristian LibangNoch keine Bewertungen
- National Monuments: The 1763 Monument Is Located in The Square of TheDokument3 SeitenNational Monuments: The 1763 Monument Is Located in The Square of TheReshana SimonNoch keine Bewertungen
- Standard Soil Test Methods & Guidelines For Interpretation of Soil ResultsDokument8 SeitenStandard Soil Test Methods & Guidelines For Interpretation of Soil ResultsReshana SimonNoch keine Bewertungen
- The Water CycleDokument5 SeitenThe Water CycleReshana SimonNoch keine Bewertungen
- Tutorial 9 The Sulfur Cycle Consists of Various Terrestrial and Atmospheric Processes Consisting of Different Oxidation and Reduction ReactionDokument2 SeitenTutorial 9 The Sulfur Cycle Consists of Various Terrestrial and Atmospheric Processes Consisting of Different Oxidation and Reduction ReactionReshana SimonNoch keine Bewertungen
- Ok Ale Boet Al ManualDokument131 SeitenOk Ale Boet Al ManualJaimeNoch keine Bewertungen
- Bio Tutorial RespirationDokument3 SeitenBio Tutorial RespirationReshana SimonNoch keine Bewertungen
- Rules For Biological DrawingsDokument1 SeiteRules For Biological DrawingsReshana SimonNoch keine Bewertungen
- EnergeticsDokument1 SeiteEnergeticsJazminie OsborneNoch keine Bewertungen
- Mass SpectrosDokument48 SeitenMass SpectrosReshana SimonNoch keine Bewertungen
- The Production of Sulphuric AcidDokument1 SeiteThe Production of Sulphuric AcidReshana SimonNoch keine Bewertungen
- CAPE Biology Unit 1 Multiple Choice Answers KeyDokument1 SeiteCAPE Biology Unit 1 Multiple Choice Answers KeyReshana SimonNoch keine Bewertungen
- CAPE Biology U1 P1 AnswersDokument2 SeitenCAPE Biology U1 P1 AnswersReshana SimonNoch keine Bewertungen
- The Notting Hill CarnivalDokument2 SeitenThe Notting Hill CarnivalReshana SimonNoch keine Bewertungen
- CAPE Laboratory Report FormatDokument3 SeitenCAPE Laboratory Report FormatReshana Simon100% (1)
- EnergeticsDokument1 SeiteEnergeticsJazminie OsborneNoch keine Bewertungen
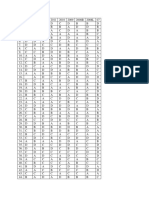
- Cape Biology Multiple Choice Answer SheetsDokument2 SeitenCape Biology Multiple Choice Answer SheetsReshana SimonNoch keine Bewertungen
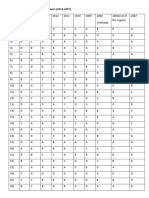
- CAPE Communication Studies 2014-U1-P2Dokument6 SeitenCAPE Communication Studies 2014-U1-P2Reshana Simon100% (1)
- CAPE Communication Studies-2019-U1-P1 PDFDokument11 SeitenCAPE Communication Studies-2019-U1-P1 PDFReshana SimonNoch keine Bewertungen
- Physical PropertiesDokument1 SeitePhysical PropertiesJazminie OsborneNoch keine Bewertungen
- U1 Biology Multiple Choice AnswersDokument2 SeitenU1 Biology Multiple Choice AnswersReshana SimonNoch keine Bewertungen
- 2017 PDFDokument19 Seiten2017 PDFkareshmaNoch keine Bewertungen
- CAPE Communication Studies 2015 P1-1 PDFDokument13 SeitenCAPE Communication Studies 2015 P1-1 PDFamrit40% (5)
- Volumetric Methods Analysis GuideDokument46 SeitenVolumetric Methods Analysis GuideReshana SimonNoch keine Bewertungen
- Determination of The Formula of Hydrated Magnesium Sulfate ActivityDokument3 SeitenDetermination of The Formula of Hydrated Magnesium Sulfate ActivityReshana SimonNoch keine Bewertungen
- CAPEDokument12 SeitenCAPENavindra Jaggernauth100% (1)
- CAPE Communication Studies 2003 P1 PDFDokument9 SeitenCAPE Communication Studies 2003 P1 PDFRiaz JokanNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Artificial Birth ControlDokument4 SeitenArtificial Birth Controljessa tabanginNoch keine Bewertungen
- Practical Gynecology 221002 234708Dokument44 SeitenPractical Gynecology 221002 234708Muhammad RizgarNoch keine Bewertungen
- RITIKA MALHOTRA, 7056, Zoology Hons., 3rd Sem, 2nd Yr, Assignment On Female Contraception PDFDokument42 SeitenRITIKA MALHOTRA, 7056, Zoology Hons., 3rd Sem, 2nd Yr, Assignment On Female Contraception PDFritika malhotraNoch keine Bewertungen
- Birth ControlDokument42 SeitenBirth ControlSelang PastNoch keine Bewertungen
- Uts - Lesson 4 and 5Dokument16 SeitenUts - Lesson 4 and 5Jwhll MaeNoch keine Bewertungen
- IUD Aftercare InstructionsDokument2 SeitenIUD Aftercare InstructionsTorsha GhoshNoch keine Bewertungen
- Intrauterine Device - WikipediaDokument80 SeitenIntrauterine Device - WikipediaDarshan MvNoch keine Bewertungen
- Female SterilizationDokument6 SeitenFemale Sterilizationjkj;jjNoch keine Bewertungen
- Family Planning Methods Comparison: IUDs vs ImplantsDokument46 SeitenFamily Planning Methods Comparison: IUDs vs ImplantsBrainy GamerARNoch keine Bewertungen
- Iud Pamphlet June 2015Dokument2 SeitenIud Pamphlet June 2015Aprilihardini LaksmiNoch keine Bewertungen
- The 5 Kinds of IUD Birth Control and Their Side EffectsDokument27 SeitenThe 5 Kinds of IUD Birth Control and Their Side EffectsGladie Ann Dela RosaNoch keine Bewertungen
- Journal Expulsion of IUDDokument12 SeitenJournal Expulsion of IUDericNoch keine Bewertungen
- Scope and Standards of Maternal Child NursingDokument41 SeitenScope and Standards of Maternal Child NursingPrincess Vanquiray100% (1)
- Intrauterine Contraception: ReviewDokument9 SeitenIntrauterine Contraception: ReviewSaeed HasanNoch keine Bewertungen
- Iud PPT ColorDokument47 SeitenIud PPT ColorYonaziraNoch keine Bewertungen
- Postpartum Period 1Dokument93 SeitenPostpartum Period 1Angela Joy AmparadoNoch keine Bewertungen
- Contraception Method1Dokument24 SeitenContraception Method1jyoti singhNoch keine Bewertungen
- Contraception UpdateDokument24 SeitenContraception UpdatePSmNoch keine Bewertungen
- Teaching Methods and Evaluation in Family PlanningDokument9 SeitenTeaching Methods and Evaluation in Family PlanningDeepika PatidarNoch keine Bewertungen
- CALM Contraception Lesson 1Dokument26 SeitenCALM Contraception Lesson 1So Eun MinNoch keine Bewertungen
- Essential IUD Birth Control Consent (39Dokument1 SeiteEssential IUD Birth Control Consent (39risa nuradilaNoch keine Bewertungen
- IUD Information: Reproductive Health Access Project / March 2017Dokument2 SeitenIUD Information: Reproductive Health Access Project / March 2017yohanasmjtNoch keine Bewertungen
- Family PlanningDokument6 SeitenFamily PlanningfsdfasfasNoch keine Bewertungen
- Contraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Dokument23 SeitenContraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Sitha MahendrataNoch keine Bewertungen
- IUD Take-Home Sheet: XXXXXX Health CenterDokument1 SeiteIUD Take-Home Sheet: XXXXXX Health Centerdoppler_Noch keine Bewertungen
- Case Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureDokument9 SeitenCase Report: Retained Intrauterine Device (IUD) : Triple Case Report and Review of The LiteratureYosie Yulanda PutraNoch keine Bewertungen
- Oral Contraceptive PillDokument21 SeitenOral Contraceptive Pilljuly3ciaNoch keine Bewertungen
- Reproductive Health Bill (HB 96) Ethical Analysis and Objections With Abstract Publication Edition - Fr. Joaquin Ferrer SVD, PH.DDokument30 SeitenReproductive Health Bill (HB 96) Ethical Analysis and Objections With Abstract Publication Edition - Fr. Joaquin Ferrer SVD, PH.DCarlos Antonio P. Palad100% (1)
- IUD Consent Form ExplainedDokument2 SeitenIUD Consent Form ExplainedShelly PierceNoch keine Bewertungen
- IUD Aftercare InstructionsDokument2 SeitenIUD Aftercare Instructionswhiterose08Noch keine Bewertungen