Das könnte Ihnen auch gefallen
- The Problem and Its BackgroundDokument78 SeitenThe Problem and Its BackgroundYette Polillo Conde0% (1)
- Nicu NCPDokument2 SeitenNicu NCPYette Polillo Conde100% (1)
- Nursing Care Plan (Ineffective Breathing Pattern)Dokument1 SeiteNursing Care Plan (Ineffective Breathing Pattern)Michael Vincent DuroNoch keine Bewertungen
- NCPDokument8 SeitenNCPYette Polillo CondeNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Baba RamdevDokument8 SeitenBaba RamdevMogul MagnateNoch keine Bewertungen
- Complete Head To Toe Procedure ChecklistDokument10 SeitenComplete Head To Toe Procedure ChecklistGeno Adrian T PampangaNoch keine Bewertungen
- CPR and First Aid Guidelines: Presentation Prepared By: Randy G. Tabaog, LPT AMA Computer College Santiago CampusDokument24 SeitenCPR and First Aid Guidelines: Presentation Prepared By: Randy G. Tabaog, LPT AMA Computer College Santiago CampussunshineNoch keine Bewertungen
- Medical PREFIXES and SUFIXESDokument52 SeitenMedical PREFIXES and SUFIXESThirdz TylerNoch keine Bewertungen
- Naturopathy 04 Air TherapyDokument64 SeitenNaturopathy 04 Air TherapymsoonNoch keine Bewertungen
- The Woman's Set KriyaDokument9 SeitenThe Woman's Set KriyaAvi MagiNoch keine Bewertungen
- Mouse DissectionDokument6 SeitenMouse DissectionMauricio F. VillamarNoch keine Bewertungen
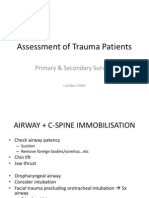
- Primary SurveyDokument19 SeitenPrimary SurveyCaroline ChauNoch keine Bewertungen
- How To Treat A Bullet Wound (With Pictures) - WikiHowDokument7 SeitenHow To Treat A Bullet Wound (With Pictures) - WikiHowOm Singh IndaNoch keine Bewertungen
- Evaluation, Tests and Measures in Physical TherapyDokument339 SeitenEvaluation, Tests and Measures in Physical TherapywanderlastNoch keine Bewertungen
- People vs. ManzanoDokument14 SeitenPeople vs. ManzanoHumility Mae FrioNoch keine Bewertungen
- Interpreting Chest FilmsDokument122 SeitenInterpreting Chest Filmsgeorgen1Noch keine Bewertungen
- Angiology NoteDokument13 SeitenAngiology NoteSantosh Bhandari100% (2)
- Cap. 06 - Avian Anatomy and PhysiologyDokument65 SeitenCap. 06 - Avian Anatomy and PhysiologyNailson JúniorNoch keine Bewertungen
- ITISMITA Biswal MSC, Nursing 2 YearDokument48 SeitenITISMITA Biswal MSC, Nursing 2 YearGandimareiNoch keine Bewertungen
- The Airway Jedi - Education On Airway Management and AnesthesiaThe Airway Jedi - Tips and Tricks On Intubation, Airway Management, Anesthesia and Safe Patient CareDokument48 SeitenThe Airway Jedi - Education On Airway Management and AnesthesiaThe Airway Jedi - Tips and Tricks On Intubation, Airway Management, Anesthesia and Safe Patient Carepradeep daniel100% (1)
- Subcutaneous: EmphysemaDokument70 SeitenSubcutaneous: EmphysemaWer TeumeNoch keine Bewertungen
- (Advait) Pranayama The Vedic Science of BreathDokument76 Seiten(Advait) Pranayama The Vedic Science of BreathASHISH K ADIGANoch keine Bewertungen
- DR V Krishna Murthy HintsDokument31 SeitenDR V Krishna Murthy HintsDrmengani Vamsi Krishna Reddy100% (2)
- OSTEOPATHIC OBSTETRICS Rev PDFDokument49 SeitenOSTEOPATHIC OBSTETRICS Rev PDFAurora Alina Bujor-FlueranNoch keine Bewertungen
- Form 3 Science Chapter 1Dokument9 SeitenForm 3 Science Chapter 1Mohamad Harith100% (1)
- Human vs. Frog Muscular System: SkeletonDokument3 SeitenHuman vs. Frog Muscular System: SkeletonRochel Labiton AlitaoNoch keine Bewertungen
- Lagier 2022Dokument31 SeitenLagier 2022Carlos Daniel AliagaNoch keine Bewertungen
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective DataDokument6 SeitenAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Evaluation Subjective DataDeinielle Magdangal RomeroNoch keine Bewertungen
- All Anatomy Mini QuestionsDokument112 SeitenAll Anatomy Mini QuestionsDiMa Marsh100% (4)
- Bingo Powerpoint v3 Answers AZCOM RadiologyDokument76 SeitenBingo Powerpoint v3 Answers AZCOM Radiologyk5c4s89Noch keine Bewertungen
- Breathing RetrainingDokument39 SeitenBreathing RetrainingAishwarya PanchalNoch keine Bewertungen
- White Dwarf Warhammer 40K CompendiumDokument200 SeitenWhite Dwarf Warhammer 40K CompendiumSadisticSeraph100% (1)
- Surgery FINAL 2023Dokument140 SeitenSurgery FINAL 2023TayaNoch keine Bewertungen
- People Vs Manzano JRDokument16 SeitenPeople Vs Manzano JRFelix Gabriel BalaniNoch keine Bewertungen