Das könnte Ihnen auch gefallen
- Cancellation of Removal for Lawful Permanent ResidentsVon EverandCancellation of Removal for Lawful Permanent ResidentsNoch keine Bewertungen
- At Altura - Move in ClearanceDokument2 SeitenAt Altura - Move in ClearancevictorcarlosliuNoch keine Bewertungen
- PSVRDokument6 SeitenPSVRSudhanshu SamalNoch keine Bewertungen
- Subject-5 Abuse FormDokument1 SeiteSubject-5 Abuse FormOke Adasen100% (2)
- Move-In Clearance Form - TRAG 2023Dokument1 SeiteMove-In Clearance Form - TRAG 2023Dominique Dela PenaNoch keine Bewertungen
- Personal Accident InsuranceDokument3 SeitenPersonal Accident InsuranceSwiftNoch keine Bewertungen
- Agreement Pertaining To Loss or Destruction of PolicyDokument2 SeitenAgreement Pertaining To Loss or Destruction of PolicyjedNoch keine Bewertungen
- Personal Accident Critical Illness Hospital Income Claim FormDokument3 SeitenPersonal Accident Critical Illness Hospital Income Claim FormHihiNoch keine Bewertungen
- Application For Certificate of ComplianceDokument2 SeitenApplication For Certificate of CompliancePan Gulf Valves ManufacturingNoch keine Bewertungen
- Arizona Game and Fish Department Solicitation / Event ApplicationDokument4 SeitenArizona Game and Fish Department Solicitation / Event ApplicationAlfonso Coronado RosasNoch keine Bewertungen
- Checklist 11222 FinalDokument2 SeitenChecklist 11222 FinalLGU BAROTAC NUEVO ESTELITA O. SUMAYONoch keine Bewertungen
- Aditya Birla - Claim - FormDokument9 SeitenAditya Birla - Claim - FormSaransh KumarNoch keine Bewertungen
- Certification Submission FormDokument2 SeitenCertification Submission FormAmenAllah DghimNoch keine Bewertungen
- Travel Claim Form (NEW)Dokument5 SeitenTravel Claim Form (NEW)HihiNoch keine Bewertungen
- 2704請求延期執行觀察勒戒聲請表Dokument3 Seiten2704請求延期執行觀察勒戒聲請表edNoch keine Bewertungen
- Form-12 Accident Report From EmployerDokument2 SeitenForm-12 Accident Report From Employersupriya100% (2)
- AIIRDokument1 SeiteAIIRNikkos BergolaNoch keine Bewertungen
- Landlord Rental ApplicationDokument2 SeitenLandlord Rental ApplicationBecky Lewis LucasNoch keine Bewertungen
- CBF 12 Motion For Issuance of TPODokument7 SeitenCBF 12 Motion For Issuance of TPOAndro DayaoNoch keine Bewertungen
- Prulife UK Application FormDokument9 SeitenPrulife UK Application FormjayarcyNoch keine Bewertungen
- Parking Sticker Application Form: Requested By: Phone / Mobile: Email: Unit / Floor: Date / HoursDokument1 SeiteParking Sticker Application Form: Requested By: Phone / Mobile: Email: Unit / Floor: Date / HoursMey SarahNoch keine Bewertungen
- Register of InjuryDokument3 SeitenRegister of InjurypenichopsNoch keine Bewertungen
- Group Claim Form (Non-Employer - Employee) : (DD/MM/YYYY) (DD/MM/YYYY) (DD/MM/YYYY)Dokument3 SeitenGroup Claim Form (Non-Employer - Employee) : (DD/MM/YYYY) (DD/MM/YYYY) (DD/MM/YYYY)ViveksomuNoch keine Bewertungen
- Death Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3Dokument3 SeitenDeath Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3vertine belerNoch keine Bewertungen
- GsisDokument3 SeitenGsisPecu MT ProvinceNoch keine Bewertungen
- Medicash Claim FormDokument6 SeitenMedicash Claim Formwaran RMNoch keine Bewertungen
- 1414 - 01 - Form 1 - Bidder's Qualification DataDokument3 Seiten1414 - 01 - Form 1 - Bidder's Qualification DataOQC PetroleumNoch keine Bewertungen
- ELIB Group Claims Claimant Statement FormDokument2 SeitenELIB Group Claims Claimant Statement FormPnk Telok KemangNoch keine Bewertungen
- Demolition FormsDokument5 SeitenDemolition Formslorie.cwe18Noch keine Bewertungen
- Request For Cashless HospitalisationDokument3 SeitenRequest For Cashless HospitalisationJegatheswaran MNoch keine Bewertungen
- Health Claim Form Part-BDokument3 SeitenHealth Claim Form Part-BAnkit KanojiaNoch keine Bewertungen
- Agent RequirementsDokument5 SeitenAgent RequirementsamericaategaNoch keine Bewertungen
- XPCR SourcingDokument1 SeiteXPCR Sourcinghrithik_169116316Noch keine Bewertungen
- MedicalDokument5 SeitenMedicalankur parekhNoch keine Bewertungen
- Application For Occupancy: Form Valid For Georgia Apartment Association Members OnlyDokument4 SeitenApplication For Occupancy: Form Valid For Georgia Apartment Association Members OnlyPatricia WellsNoch keine Bewertungen
- Birth Affidavit: Last Suffix First MiddleDokument2 SeitenBirth Affidavit: Last Suffix First Middlesidiki millimonoNoch keine Bewertungen
- Minnesota Rental Application FormDokument2 SeitenMinnesota Rental Application FormJonathan McNallyNoch keine Bewertungen
- Liability Claim FormDokument3 SeitenLiability Claim FormHihiNoch keine Bewertungen
- Ec 04Dokument2 SeitenEc 04Natnael SolomonNoch keine Bewertungen
- Claim Form - Part-B - HospitalDokument4 SeitenClaim Form - Part-B - HospitalMadhavi BobadeNoch keine Bewertungen
- Health Claim - Form-1Dokument5 SeitenHealth Claim - Form-1Pinakin PatelNoch keine Bewertungen
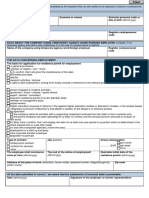
- I Confirm, That I Will Grant The Maintenance of The Alien: or Date of Birth (Dd/mm/yyyy)Dokument2 SeitenI Confirm, That I Will Grant The Maintenance of The Alien: or Date of Birth (Dd/mm/yyyy)sensationNoch keine Bewertungen
- Employee Medical Incident ReportDokument1 SeiteEmployee Medical Incident ReportAiswarya SukumarNoch keine Bewertungen
- ApolloMunich-Easy HealthDokument9 SeitenApolloMunich-Easy HealthRS CharyNoch keine Bewertungen
- Fill-In - License Application FormDokument9 SeitenFill-In - License Application FormRechelle Anne Soriano-MagsinoNoch keine Bewertungen
- Group Medi Prime ClaimFormDokument6 SeitenGroup Medi Prime ClaimFormPravin Balasaheb GunjalNoch keine Bewertungen
- Range Instructors CertificationDokument5 SeitenRange Instructors CertificationDavion Essens BrittonNoch keine Bewertungen
- Resident Info Sheet 2023Dokument1 SeiteResident Info Sheet 2023v.william.zhengNoch keine Bewertungen
- NTUC Pa Paid Claim Form (08 2017)Dokument5 SeitenNTUC Pa Paid Claim Form (08 2017)pat5355Noch keine Bewertungen
- Temporary Workmen FormDokument1 SeiteTemporary Workmen FormMR. MANTU DWIVEDINoch keine Bewertungen
- Know Yor Customer - Addendum: (For Third Party Payment)Dokument2 SeitenKnow Yor Customer - Addendum: (For Third Party Payment)Shrikant GawhaneNoch keine Bewertungen
- CLEIC Application Form 072010Dokument2 SeitenCLEIC Application Form 072010Vintonius Raffaele PRIMUSNoch keine Bewertungen
- SUBP-001 FormDokument2 SeitenSUBP-001 FormpratyusharaviNoch keine Bewertungen
- 0811 Ma App Form Version 190 1Dokument3 Seiten0811 Ma App Form Version 190 1vmjjc7jtg2Noch keine Bewertungen
- NM Self/Participant Direction Pre-Hire Packet: Criminal History Authorization For Release of Information (Required)Dokument7 SeitenNM Self/Participant Direction Pre-Hire Packet: Criminal History Authorization For Release of Information (Required)ShellyJacksonNoch keine Bewertungen
- Hospital Benefit Claim Form: Part I: Claimant'S StatementDokument4 SeitenHospital Benefit Claim Form: Part I: Claimant'S StatementyleeNoch keine Bewertungen
- FLA001A-Application For Firearm Licences Certificates and Permits - June 2020Dokument2 SeitenFLA001A-Application For Firearm Licences Certificates and Permits - June 2020dilanNoch keine Bewertungen
- Death Claim FormDokument4 SeitenDeath Claim FormudufkhkfysfkgoNoch keine Bewertungen
- Appendix-V Form-I Application For Obtaining Disability Certificate by Persons With Disabilities (See Rule 3)Dokument7 SeitenAppendix-V Form-I Application For Obtaining Disability Certificate by Persons With Disabilities (See Rule 3)Facebook Verification TeamNoch keine Bewertungen
- Death Claim Form PDFDokument4 SeitenDeath Claim Form PDFSupdt. of Post offices Kanpur (M) Dn. KanpurNoch keine Bewertungen
- How To Write An Informal ArticleDokument1 SeiteHow To Write An Informal ArticleDS SystemsNoch keine Bewertungen
- Employee Incident Report FormDokument2 SeitenEmployee Incident Report FormDS SystemsNoch keine Bewertungen
- Workplace Incident Report FormDokument2 SeitenWorkplace Incident Report FormDS SystemsNoch keine Bewertungen
- Writing Articles The Quick and Easy WayDokument1 SeiteWriting Articles The Quick and Easy WayDS SystemsNoch keine Bewertungen
- What Is An Article With DefinitionsDokument1 SeiteWhat Is An Article With DefinitionsDS SystemsNoch keine Bewertungen
- How To Write Review PaperDokument2 SeitenHow To Write Review PaperTasneem Vahora100% (1)
- Articles On Toddlers or Home RepairsDokument1 SeiteArticles On Toddlers or Home RepairsDS SystemsNoch keine Bewertungen
- Expense Reimbursement ReportDokument1 SeiteExpense Reimbursement ReportDS SystemsNoch keine Bewertungen
- Structuring An ArticleDokument1 SeiteStructuring An ArticleDS SystemsNoch keine Bewertungen
- Sample Medical Incident Report: Section 1Dokument2 SeitenSample Medical Incident Report: Section 1DS SystemsNoch keine Bewertungen
- Annotated Case Report FormDokument5 SeitenAnnotated Case Report FormDS SystemsNoch keine Bewertungen
- Three Cover Bid Submission New v906 PDFDokument61 SeitenThree Cover Bid Submission New v906 PDFDS SystemsNoch keine Bewertungen
- Sample Medical Incident Report: Section 1Dokument2 SeitenSample Medical Incident Report: Section 1DS SystemsNoch keine Bewertungen
- Electronic Patient Report FormDokument6 SeitenElectronic Patient Report FormDS Systems0% (1)
- Bid Withdrawal Updated v906Dokument20 SeitenBid Withdrawal Updated v906sombansNoch keine Bewertungen
- Case Report Consent FormDokument1 SeiteCase Report Consent FormDS SystemsNoch keine Bewertungen
- Auto Accident Report FormDokument2 SeitenAuto Accident Report FormDS SystemsNoch keine Bewertungen
- Bidder Registration Manual Updated v906Dokument60 SeitenBidder Registration Manual Updated v906Sunil rathoreNoch keine Bewertungen
- DownloadForMac SanDiskSecureAccessV3.0Dokument1 SeiteDownloadForMac SanDiskSecureAccessV3.0Gherca OvidiuNoch keine Bewertungen
- Enquiry Updated v906Dokument23 SeitenEnquiry Updated v906gurpreets_807665Noch keine Bewertungen
- Government System Of: National Informatics CentreDokument35 SeitenGovernment System Of: National Informatics CentreDS SystemsNoch keine Bewertungen
- 3 PaymentDokument6 Seiten3 PaymentSwathi Sunder KNoch keine Bewertungen
- Difference Between HR & AdminDokument3 SeitenDifference Between HR & AdminDS SystemsNoch keine Bewertungen
- ECR For Employers File StructureDokument2 SeitenECR For Employers File StructureRajeshsatya LankaNoch keine Bewertungen
- Three Cover Bid Submission New v906 PDFDokument61 SeitenThree Cover Bid Submission New v906 PDFDS SystemsNoch keine Bewertungen
- Time ManagementDokument1 SeiteTime ManagementDS SystemsNoch keine Bewertungen
- Two 1 Cover Bid Submission New v906Dokument59 SeitenTwo 1 Cover Bid Submission New v906asd123412Noch keine Bewertungen
- Various Type of EmployeeDokument1 SeiteVarious Type of EmployeeDS SystemsNoch keine Bewertungen
- Frequently Encountered Problems and SolutionsDokument4 SeitenFrequently Encountered Problems and SolutionsDS SystemsNoch keine Bewertungen
- Doctor QuotesDokument5 SeitenDoctor Quotesapi-303147801Noch keine Bewertungen
- The Association of Philippine Physicians in MarylandDokument32 SeitenThe Association of Philippine Physicians in Marylandjoy in the spirit of the lordNoch keine Bewertungen
- Become A Clinical ExpertiseDokument12 SeitenBecome A Clinical ExpertiseIsmael Vara CarvalhoNoch keine Bewertungen
- Reason and Impartiality As Minimum Requirement For MoralityDokument6 SeitenReason and Impartiality As Minimum Requirement For MoralityKimchi Haru91% (23)
- Pro-Choice Violence in OntarioDokument16 SeitenPro-Choice Violence in OntarioHuman Life InternationalNoch keine Bewertungen
- Complementary and Alternative TherapiesDokument16 SeitenComplementary and Alternative TherapiesHannah Jean Lapenid LemorenasNoch keine Bewertungen
- PMD Permanent RegistrationDokument3 SeitenPMD Permanent RegistrationTouheed KhalidNoch keine Bewertungen
- Contextualized Module and Activity of Creative Non-Fiction 4TH QRTRDokument7 SeitenContextualized Module and Activity of Creative Non-Fiction 4TH QRTRremely marcosNoch keine Bewertungen
- Curriculum AvedisDokument20 SeitenCurriculum Avedissyarifah mawaddahNoch keine Bewertungen
- 2025: 20% Doctor Included? An Exercise in Technology Speculation & MusingsDokument49 Seiten2025: 20% Doctor Included? An Exercise in Technology Speculation & MusingsTransform Healthcare ITNoch keine Bewertungen
- Detailed Lesson Plan in Musical PlayDokument9 SeitenDetailed Lesson Plan in Musical PlayJovelyn TakilidNoch keine Bewertungen
- Midwifery Scope of PracticeDokument4 SeitenMidwifery Scope of PracticeHeather Dalton100% (1)
- Botanic Drugs Their 1000081906Dokument400 SeitenBotanic Drugs Their 1000081906adiseifNoch keine Bewertungen
- 17 Soc - Sec.rep - Ser. 788, Medicare&medicaid Gu 36,323 George Friedman v. Secretary of The Department of Health and Human Services, 819 F.2d 42, 2d Cir. (1987)Dokument7 Seiten17 Soc - Sec.rep - Ser. 788, Medicare&medicaid Gu 36,323 George Friedman v. Secretary of The Department of Health and Human Services, 819 F.2d 42, 2d Cir. (1987)Scribd Government DocsNoch keine Bewertungen
- Enrolled Nurses FADokument11 SeitenEnrolled Nurses FAjoayou23Noch keine Bewertungen
- Introduction To Family Medicine: Principles, Concepts and PracticeDokument41 SeitenIntroduction To Family Medicine: Principles, Concepts and PracticeZaqueo Gutierrez FajardoNoch keine Bewertungen
- Resumesssss 2017Dokument3 SeitenResumesssss 2017api-351156642Noch keine Bewertungen
- MdayurDokument88 SeitenMdayurIoan-ovidiu Cordis0% (1)
- Tribute of The Nigerian Council of Physicians of Natural Medicine To Prof. Archbishop Magnus Adeyemi Atilade Written by Prof. Gilbert EzengigeDokument2 SeitenTribute of The Nigerian Council of Physicians of Natural Medicine To Prof. Archbishop Magnus Adeyemi Atilade Written by Prof. Gilbert EzengigeOgonna AnyigadiNoch keine Bewertungen
- Pharm - Min11706 - Early RefillDokument22 SeitenPharm - Min11706 - Early RefillJames LindonNoch keine Bewertungen
- Right To Informed ConsentDokument2 SeitenRight To Informed ConsentRusty NomadNoch keine Bewertungen
- Califronia Medical Asoociates CMAOnCall1315Dokument25 SeitenCalifronia Medical Asoociates CMAOnCall1315Richard BrumfieldNoch keine Bewertungen
- Hifu Facelift Singapore - DR Chua Cheng YuDokument9 SeitenHifu Facelift Singapore - DR Chua Cheng YuHifu Singapore - Dr Chua Cheng YuNoch keine Bewertungen
- Ida Jean Orlando - SoftDokument5 SeitenIda Jean Orlando - SoftBenjamin TanNoch keine Bewertungen
- Bajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdDokument2 SeitenBajaj Allianz General Insurance Company Limited: Claim Form - Domiciliary and OpdvkbasavaNoch keine Bewertungen
- Doctor Job Description Position Title DoctorDokument4 SeitenDoctor Job Description Position Title DoctorBianca Andreea BalintNoch keine Bewertungen
- Primegala Med ProfileDokument3 SeitenPrimegala Med Profilestephen oriediNoch keine Bewertungen
- Evidence Based in Rheumatology PDFDokument364 SeitenEvidence Based in Rheumatology PDFFanie BeatriceNoch keine Bewertungen
- Analysis of A Us Health Care PolicyDokument6 SeitenAnalysis of A Us Health Care Policyapi-470941612Noch keine Bewertungen
- Doctor - Patient RelationshipDokument32 SeitenDoctor - Patient RelationshipRushdaNoch keine Bewertungen