Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Pro-Social Behavior in Rats Is Modulated by Social ExperienceDokument16 SeitenPro-Social Behavior in Rats Is Modulated by Social ExperienceCarolina ValenciaNoch keine Bewertungen
- Reducing The Cost of Dissociative Identity Disorder Measuring The EffectivenessDokument10 SeitenReducing The Cost of Dissociative Identity Disorder Measuring The EffectivenessCarolina ValenciaNoch keine Bewertungen
- Content ServerDokument5 SeitenContent ServerCarolina ValenciaNoch keine Bewertungen
- SARS Control and Psychological Effects of QuarentineDokument2 SeitenSARS Control and Psychological Effects of QuarentineCarolina ValenciaNoch keine Bewertungen
- Lazarus2019 Article TooMuchTooSoonBorderlinePersonDokument11 SeitenLazarus2019 Article TooMuchTooSoonBorderlinePersonCarolina ValenciaNoch keine Bewertungen
- Is Borderline Personality Disorder A Serious Mental Illness?Dokument7 SeitenIs Borderline Personality Disorder A Serious Mental Illness?Carolina ValenciaNoch keine Bewertungen
- Loneliness, Social Networks, and Social Functioning in Borderline Personality DisorderDokument10 SeitenLoneliness, Social Networks, and Social Functioning in Borderline Personality DisorderCarolina ValenciaNoch keine Bewertungen
- Definitions: Diagnosis and Comorbidity: Diagnostic and Statistical Manual of Mental Disorders, Fourth EditionDokument13 SeitenDefinitions: Diagnosis and Comorbidity: Diagnostic and Statistical Manual of Mental Disorders, Fourth EditionCarolina ValenciaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- TNPCB PDFDokument231 SeitenTNPCB PDFGunaseelan RvNoch keine Bewertungen
- GA1 4 Bach Inglés NV 2021 - Luz Daniela Real MerlosDokument2 SeitenGA1 4 Bach Inglés NV 2021 - Luz Daniela Real Merlosluz Daniela Real MerlosNoch keine Bewertungen
- VersaLink C405 Service ManualDokument858 SeitenVersaLink C405 Service ManualAlex Rodriguez BarronNoch keine Bewertungen
- TDS Simacover EP Buildcoat (Intermediate)Dokument2 SeitenTDS Simacover EP Buildcoat (Intermediate)rrahardiandiasNoch keine Bewertungen
- Page 2 Positive Psychology Page 3 Jan D. Sinnott Editor Positive Psychology Advances in ...Dokument358 SeitenPage 2 Positive Psychology Page 3 Jan D. Sinnott Editor Positive Psychology Advances in ...Javed67% (3)
- Module 2 Ethics and Culture-3Dokument26 SeitenModule 2 Ethics and Culture-3Charles Ronald GenatoNoch keine Bewertungen
- Plate Tectonics Gizmo Form PDFDokument5 SeitenPlate Tectonics Gizmo Form PDFJorge Cota85% (13)
- Biomedical Waste ManagementDokument39 SeitenBiomedical Waste ManagementSeema TanvirNoch keine Bewertungen
- DENTISTRY Assessment of Fundamental Knowledge 2014Dokument10 SeitenDENTISTRY Assessment of Fundamental Knowledge 2014sarookaNoch keine Bewertungen
- FZK k2 BHGN BDokument8 SeitenFZK k2 BHGN BAdyfairos NayahNoch keine Bewertungen
- Total Selected ListDokument32 SeitenTotal Selected ListVamsi KrishnaNoch keine Bewertungen
- Sarah Bond: HR Assistant ResumeDokument3 SeitenSarah Bond: HR Assistant ResumeKv kNoch keine Bewertungen
- Ice Slurry Applications PDFDokument15 SeitenIce Slurry Applications PDFmattiturboNoch keine Bewertungen
- 076 Fujifilm Motion Picture Film ManualDokument40 Seiten076 Fujifilm Motion Picture Film ManualPatricio A. Mancilla RiosecoNoch keine Bewertungen
- FinalDokument1 SeiteFinalAbas AcmadNoch keine Bewertungen
- Assignment3 BscProjectDokument12 SeitenAssignment3 BscProjectBernard BrinkelNoch keine Bewertungen
- Unit 9 - Test 2Dokument4 SeitenUnit 9 - Test 2Dương Mai ThùyNoch keine Bewertungen
- Pazzaglia 2013Dokument34 SeitenPazzaglia 2013João Carlos CerqueiraNoch keine Bewertungen
- IS 513 Grade EDDDokument2 SeitenIS 513 Grade EDDRamji GautamNoch keine Bewertungen
- Deep LearningDokument189 SeitenDeep LearningmausamNoch keine Bewertungen
- Jhepgc 2024020817174319Dokument46 SeitenJhepgc 2024020817174319staszkxyNoch keine Bewertungen
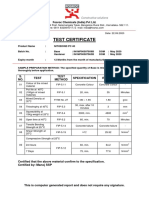
- Test Certificate: S. NO. Test Test Method Specification Result UOMDokument1 SeiteTest Certificate: S. NO. Test Test Method Specification Result UOMkaushik100% (1)
- Etsa V3Dokument18 SeitenEtsa V3Robbani HamdanNoch keine Bewertungen
- 3BSE001974R601Dokument174 Seiten3BSE001974R601Clayton100% (1)
- Anthropology and The Changing WorldDokument12 SeitenAnthropology and The Changing Worldbilal1710Noch keine Bewertungen
- Methods For Describing Sets of DataDokument114 SeitenMethods For Describing Sets of DataJuan FranNoch keine Bewertungen
- En Mi Cuerpo SientoDokument33 SeitenEn Mi Cuerpo Sientofresky2Noch keine Bewertungen
- Time ManagementDokument4 SeitenTime ManagementBanupriya BalasubramanianNoch keine Bewertungen
- English Composition IDokument6 SeitenEnglish Composition ILeo GonellNoch keine Bewertungen
- 2024 GR 12 PROJECT(5)Dokument7 Seiten2024 GR 12 PROJECT(5)dimphoboledi13100% (1)