Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Kawasaki Disease-Case-Study LATEST CHANGESDokument24 SeitenKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Introduction To Pharmaceutical MicrobiologyDokument35 SeitenIntroduction To Pharmaceutical MicrobiologylorrainebarandonNoch keine Bewertungen
- Philippines Commitment Self-Reporting Questionnaire 2018Dokument7 SeitenPhilippines Commitment Self-Reporting Questionnaire 2018JOSHUA DICHOSONoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Ge 8 - Ethics: AnalysisDokument3 SeitenGe 8 - Ethics: AnalysisJOSHUA DICHOSONoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDokument19 SeitenAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
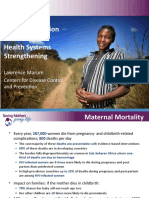
- Blood Transfusion Services and Health Systems Strengthening: Lawrence MarumDokument19 SeitenBlood Transfusion Services and Health Systems Strengthening: Lawrence MarumJOSHUA DICHOSONoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDokument2 SeitenCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- (.-..-.)Dokument1 Seite(.-..-.)JOSHUA DICHOSONoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Case PresentationDokument39 SeitenCase PresentationJOSHUA DICHOSONoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Pneumonia Presenting As Acute Abdomen in Children: A Report" of Three CasesDokument4 SeitenPneumonia Presenting As Acute Abdomen in Children: A Report" of Three CasesJOSHUA DICHOSONoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- CHN ConceptsDokument48 SeitenCHN ConceptsJOSHUA DICHOSONoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Patient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)Dokument28 SeitenPatient Positioning (Sims, Orthopneic, Dorsal Recumbent) Guide (2020)JOSHUA DICHOSO100% (1)
- Which of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsDokument2 SeitenWhich of The Statements Explains The Saying "All Work and No Play Make Jack A Dull Boy." 2 PointsJOSHUA DICHOSONoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 6234-Article Text-8420-2-10-20170221Dokument3 Seiten6234-Article Text-8420-2-10-20170221Jenry Himawan SinagaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Tobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsDokument104 SeitenTobacco Use and Second-Hand Smoke Exposure in Pregnancy: WHO RecommendationsJOSHUA DICHOSONoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Recommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseDokument34 SeitenRecommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseJOSHUA DICHOSONoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Case Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesDokument2 SeitenCase Study: Kawasaki Disease: The Heart Center Section of Infectious DiseasesJOSHUA DICHOSONoch keine Bewertungen
- Physiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFDokument15 SeitenPhysiological Rationale and Current Evidence For Therapeutic Positioning of Critically Ill Patients PDFnurulanisa0703Noch keine Bewertungen
- P롶허ㅓㅠㄹ포ㅗ)Dokument19 SeitenP롶허ㅓㅠㄹ포ㅗ)JOSHUA DICHOSONoch keine Bewertungen
- Advances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVDokument19 SeitenAdvances in Medicine and Biology', Volume 67, 2013 Nova Science Publisher Inc., Editor: Berhardt LVJOSHUA DICHOSONoch keine Bewertungen
- Introduction PDFDokument1 SeiteIntroduction PDFJOSHUA DICHOSONoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Maintaining Skin Integrity and Preventing Pressure Ulcers - Information For Nursing Care Homes - January 2018 Final v1.0Dokument29 SeitenMaintaining Skin Integrity and Preventing Pressure Ulcers - Information For Nursing Care Homes - January 2018 Final v1.0JOSHUA DICHOSO100% (1)
- Nursing Interventions and Rationales - Impaired Skin IntegrityDokument11 SeitenNursing Interventions and Rationales - Impaired Skin IntegrityJOSHUA DICHOSONoch keine Bewertungen
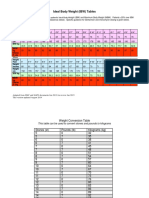
- IBW TableDokument2 SeitenIBW TablegrafikeyesNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- How To Study Pharmacology Checklist Cheat SheetDokument4 SeitenHow To Study Pharmacology Checklist Cheat SheetJOSHUA DICHOSONoch keine Bewertungen
- Nursing Care Plan (NCP) - Ultimate Guide and Database - NurseslabsDokument23 SeitenNursing Care Plan (NCP) - Ultimate Guide and Database - NurseslabsJOSHUA DICHOSONoch keine Bewertungen
- 3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsDokument12 Seiten3 Pressure Ulcer (Bedsores) Nursing Care Plans - NurseslabsJOSHUA DICHOSONoch keine Bewertungen
- Course Syllabus: Course: Hours: Course DescriptionDokument10 SeitenCourse Syllabus: Course: Hours: Course DescriptionJOSHUA DICHOSONoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Agency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3Dokument2 SeitenAgency Visit Bureau of Fire Protection Sorsogon City: Joshua C. Dichoso 1BSN3JOSHUA DICHOSONoch keine Bewertungen
- De Nition: Chapter 46 Chest ExaminationDokument7 SeitenDe Nition: Chapter 46 Chest ExaminationJOSHUA DICHOSONoch keine Bewertungen
- Applied Animal Behaviour ScienceDokument10 SeitenApplied Animal Behaviour ScienceJosé Alberto León HernándezNoch keine Bewertungen
- School Functions and School EffectivenessDokument14 SeitenSchool Functions and School EffectivenessCiku Biku100% (1)
- HCI Chapter 1Dokument23 SeitenHCI Chapter 1AschenakiNoch keine Bewertungen
- New Perspectives On Young Children's Moral Education: Developing Character Through A Virtue Ethics ApproachDokument4 SeitenNew Perspectives On Young Children's Moral Education: Developing Character Through A Virtue Ethics ApproachIcha WijayantiNoch keine Bewertungen
- English Ii: Compiled by Satya PermadiDokument16 SeitenEnglish Ii: Compiled by Satya PermadiPplp Pansophia SingarajaNoch keine Bewertungen
- Scientific American MIND, Vol. 32.1 (January-February 2021)Dokument40 SeitenScientific American MIND, Vol. 32.1 (January-February 2021)Aladin1972Noch keine Bewertungen
- Microsoft Power Point - Managing StressDokument8 SeitenMicrosoft Power Point - Managing StressMohit GautamNoch keine Bewertungen
- The Looking Glass Self BotanywaybootDokument1 SeiteThe Looking Glass Self BotanywaybootRanie MonteclaroNoch keine Bewertungen
- Unit Plan Moving Forward With The Past My Family My History and My CommunityDokument4 SeitenUnit Plan Moving Forward With The Past My Family My History and My Communityapi-649393436Noch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Earning Units Exam Principles of TeachingDokument1 SeiteEarning Units Exam Principles of TeachingJane SantiagoNoch keine Bewertungen
- Communication Is Simply The Act of Transferring Information From One Place, Person or Group To AnotherDokument3 SeitenCommunication Is Simply The Act of Transferring Information From One Place, Person or Group To AnotherYram GambzNoch keine Bewertungen
- Locsin - Technological Competency JerusalemDokument1 SeiteLocsin - Technological Competency JerusalemCloyd Marvin Pajas SegundoNoch keine Bewertungen
- Questionnaire On Employee MotivationDokument3 SeitenQuestionnaire On Employee MotivationKharim Beine0% (1)
- RW - DLP Critical Reading As ReasoningDokument8 SeitenRW - DLP Critical Reading As ReasoningJulieAnnLucasBagamaspad100% (6)
- lesson 14 Review Merry Christmas to you 祝你圣诞快乐 - 重点句子与语法复习Dokument19 Seitenlesson 14 Review Merry Christmas to you 祝你圣诞快乐 - 重点句子与语法复习Haeshan NiyarepolaNoch keine Bewertungen
- The Use of Project-Based Learning (PBL) in EFL Classroom: .IntroductionDokument32 SeitenThe Use of Project-Based Learning (PBL) in EFL Classroom: .IntroductionSitiumNoch keine Bewertungen
- DLL Arts Q3 W6Dokument7 SeitenDLL Arts Q3 W6Cherry Cervantes HernandezNoch keine Bewertungen
- Examiner's Report: Advanced Performance Management (APM) July 2020Dokument7 SeitenExaminer's Report: Advanced Performance Management (APM) July 2020Наиль РизвановNoch keine Bewertungen
- National Elctrical Installation CurriculumDokument34 SeitenNational Elctrical Installation CurriculumRudi FajardoNoch keine Bewertungen
- BRP Band Grading RubricDokument3 SeitenBRP Band Grading Rubricapi-296844101Noch keine Bewertungen
- Design Kickstart: Course SyllabusDokument2 SeitenDesign Kickstart: Course SyllabusRicardoNoch keine Bewertungen
- Castillon, Thessa H. - Thematic EssayDokument5 SeitenCastillon, Thessa H. - Thematic EssayThessa H. CastillonNoch keine Bewertungen
- Chatterjee, A., & Coslett, H.B. (Eds.) (2014) - The Roots of Cognitive Neuroscience. Behavioral Neurology and Neuropsychology. Oxford University Press PDFDokument431 SeitenChatterjee, A., & Coslett, H.B. (Eds.) (2014) - The Roots of Cognitive Neuroscience. Behavioral Neurology and Neuropsychology. Oxford University Press PDFReg A. Derah100% (1)
- Social Case Work Practice or Working With Individuals UNIT IIDokument78 SeitenSocial Case Work Practice or Working With Individuals UNIT IIJai Santhosh100% (1)
- Plantilla Exmaen B2 PDFDokument4 SeitenPlantilla Exmaen B2 PDFRafaelZúñigaGutiérrezNoch keine Bewertungen
- Czarniawska, Barbara Good Novels, Better Managment.Dokument343 SeitenCzarniawska, Barbara Good Novels, Better Managment.Carlos Roberto Zamora Bugueño0% (1)
- Reflection PaperDokument4 SeitenReflection Paperapi-531489457Noch keine Bewertungen
- Issue-Based Information SystemDokument10 SeitenIssue-Based Information Systembenjamin212Noch keine Bewertungen
- IntroCogNeuro Chapter 1Dokument20 SeitenIntroCogNeuro Chapter 1LidyaNoch keine Bewertungen
- Spanish MaterialsDokument3 SeitenSpanish MaterialsCarlos RodriguezNoch keine Bewertungen
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyVon EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyBewertung: 4.5 von 5 Sternen4.5/5 (263)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfVon EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfBewertung: 5 von 5 Sternen5/5 (36)
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherVon EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNoch keine Bewertungen
- The Meth Lunches: Food and Longing in an American CityVon EverandThe Meth Lunches: Food and Longing in an American CityBewertung: 5 von 5 Sternen5/5 (5)
- IF YOU SEE THEM: Young, Unhoused, and Alone in America.Von EverandIF YOU SEE THEM: Young, Unhoused, and Alone in America.Noch keine Bewertungen
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisVon EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisBewertung: 4 von 5 Sternen4/5 (4284)
- High-Risers: Cabrini-Green and the Fate of American Public HousingVon EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNoch keine Bewertungen