Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Further Information: ManualDokument44 SeitenFurther Information: Manualmina mirNoch keine Bewertungen
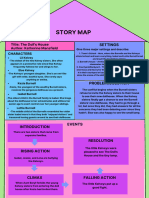
- The Doll's HouseDokument1 SeiteThe Doll's HouseanunghasauNoch keine Bewertungen
- A Collection of Post-Objectivst Essays.Dokument221 SeitenA Collection of Post-Objectivst Essays.Leo_The_Magnificent50% (2)
- Norplant: Progesterone Only ContraceptivesDokument9 SeitenNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNoch keine Bewertungen
- The First 1001 DaysDokument8 SeitenThe First 1001 DaysНиколай КотовNoch keine Bewertungen
- Parents' Lived Experiences With The COVID-19 Pandemic: Jo Lauren Weaver and Jacqueline M. SwankDokument7 SeitenParents' Lived Experiences With The COVID-19 Pandemic: Jo Lauren Weaver and Jacqueline M. SwankDarlene Dacanay DavidNoch keine Bewertungen
- 140379Dokument23 Seiten140379Naresh NelaturiNoch keine Bewertungen
- The Distance Between Us 1-5Dokument4 SeitenThe Distance Between Us 1-5api-25314052350% (2)
- Jesse Lindsey Bush (1822-1864) (Jess-1822)Dokument41 SeitenJesse Lindsey Bush (1822-1864) (Jess-1822)karen catonNoch keine Bewertungen
- Module 18: Baby Massage: by The End of This Chapter, You Will KnowDokument11 SeitenModule 18: Baby Massage: by The End of This Chapter, You Will KnowMed MedNoch keine Bewertungen
- A Meta Analysis of Effectiveness of Interventions To I - 2018 - International JoDokument12 SeitenA Meta Analysis of Effectiveness of Interventions To I - 2018 - International JoSansa LauraNoch keine Bewertungen
- Looseleaf For Experience Human Development 14Th Edition Gabriela Martorell Download PDF ChapterDokument51 SeitenLooseleaf For Experience Human Development 14Th Edition Gabriela Martorell Download PDF Chapteredward.wiseman850100% (15)
- Early Childhood Development - Chapter Three (Trawick-Smith) 2014Dokument75 SeitenEarly Childhood Development - Chapter Three (Trawick-Smith) 2014Rodney Moore67% (3)
- The Leadership Quarterly: Zhengguang Liu, Shruthi Venkatesh, Susan Elaine Murphy, Ronald E. RiggioDokument21 SeitenThe Leadership Quarterly: Zhengguang Liu, Shruthi Venkatesh, Susan Elaine Murphy, Ronald E. RiggioRupali PardasaniNoch keine Bewertungen
- Baseline Survey On Child and Related Maternal Health Care-Revised Report - Madhya Pradesh-491 - 1Dokument137 SeitenBaseline Survey On Child and Related Maternal Health Care-Revised Report - Madhya Pradesh-491 - 1National Child Health Resource Centre (NCHRC)Noch keine Bewertungen
- What Is Child PsychologyDokument16 SeitenWhat Is Child PsychologyTalha MughalNoch keine Bewertungen
- Social Skills For Teens - PEERS ProgramDokument1 SeiteSocial Skills For Teens - PEERS ProgramsocialbridgeNoch keine Bewertungen
- Chapter 1 IntroductionDokument3 SeitenChapter 1 IntroductionAiden CabanogNoch keine Bewertungen
- Jurnal BB VmiDokument9 SeitenJurnal BB VmiSarah PatimahNoch keine Bewertungen
- Issue 2Dokument3 SeitenIssue 2altaibkhan318Noch keine Bewertungen
- 6 Ways Erikson's Theory Is HelpfulDokument3 Seiten6 Ways Erikson's Theory Is Helpfulxx100% (1)
- Respiratory Distress SyndromeDokument30 SeitenRespiratory Distress SyndromeDennis MiritiNoch keine Bewertungen
- Umbilical Cord ProlapseDokument26 SeitenUmbilical Cord Prolapsesulekhaanoob100% (2)
- Ebr 1 (Ob Ii)Dokument2 SeitenEbr 1 (Ob Ii)Kathleen JosolNoch keine Bewertungen
- Chcece033 Assessment 2 Case Study 2 Alana by Rachael-Lyn AndersonDokument9 SeitenChcece033 Assessment 2 Case Study 2 Alana by Rachael-Lyn AndersonRachael-Lyn AndersonNoch keine Bewertungen
- CBT - Final Formulation PaperDokument4 SeitenCBT - Final Formulation PaperNatalia RamirezNoch keine Bewertungen
- Whitney Updated ResumeDokument2 SeitenWhitney Updated ResumeWhitney JonesNoch keine Bewertungen
- Responsible Parenthood and Reproductive Health Act of 2012Dokument22 SeitenResponsible Parenthood and Reproductive Health Act of 2012Janette Anne Reyes MacaraigNoch keine Bewertungen
- Family Structure: Family Is A Group of People orDokument24 SeitenFamily Structure: Family Is A Group of People orWiljohn de la CruzNoch keine Bewertungen
- Rukmani Kunthi: Active ThemesDokument6 SeitenRukmani Kunthi: Active ThemesImasha RavindiNoch keine Bewertungen