Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Palliative WorksheetDokument4 SeitenPalliative WorksheetrayNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- RT Triage SystemDokument4 SeitenRT Triage SystemrayNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Even/homogenous Dose Distribution Across PTV: WedgesDokument5 SeitenEven/homogenous Dose Distribution Across PTV: WedgesrayNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- ProcedureDokument13 SeitenProcedurerayNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- EK Chemistry PDFDokument364 SeitenEK Chemistry PDFray100% (8)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Rebound Returns - Asos Private Bag 211022 Laurence Stevens Drive Auckland 2154 Freepost No 252061Dokument1 SeiteRebound Returns - Asos Private Bag 211022 Laurence Stevens Drive Auckland 2154 Freepost No 252061rayNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
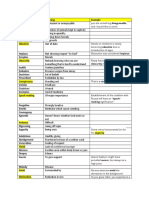
- General VocabularyDokument9 SeitenGeneral VocabularyrayNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Radt 215Dokument5 SeitenRadt 215rayNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Angry Strong Annoyance or HostilityDokument8 SeitenAngry Strong Annoyance or HostilityrayNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- MU Calc AnswersDokument2 SeitenMU Calc AnswersrayNoch keine Bewertungen
- Brain Module WorksheetDokument5 SeitenBrain Module WorksheetrayNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- RADT115 2014 Test 2 Posted On Moodle On 9 May 16Dokument5 SeitenRADT115 2014 Test 2 Posted On Moodle On 9 May 16rayNoch keine Bewertungen
- Case Study: Raymond HoveDokument20 SeitenCase Study: Raymond HoverayNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 10cm 1 10cm 1 10cm 1: Decreased FF Increased MUDokument2 Seiten10cm 1 10cm 1 10cm 1: Decreased FF Increased MUrayNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- BREAST Worksheet: Treatment Site: Right BreastDokument4 SeitenBREAST Worksheet: Treatment Site: Right BreastrayNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Radiobio EQD2 QuestionsDokument2 SeitenRadiobio EQD2 QuestionsrayNoch keine Bewertungen
- Content: Standard Operating Procedure (SOP) Use and Maintenance of An AutoclaveDokument10 SeitenContent: Standard Operating Procedure (SOP) Use and Maintenance of An Autoclaverijulesh karmelNoch keine Bewertungen
- Lac NL - Spring 2021Dokument8 SeitenLac NL - Spring 2021Ghassan NajmNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Midterm Exams NCM1531L - Care of The Older Persons LectureDokument50 SeitenMidterm Exams NCM1531L - Care of The Older Persons Lecturejjmaxh20Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Tips and Guidelines For Being A Successful ResearcherDokument11 SeitenTips and Guidelines For Being A Successful ResearcherMaria Carmela DomocmatNoch keine Bewertungen
- Mackpro WLW1Dokument1 SeiteMackpro WLW1Saeed AhmedNoch keine Bewertungen
- Dis-Infection With Ozone SystemDokument6 SeitenDis-Infection With Ozone SystemSwaminathan ThayumanavanNoch keine Bewertungen
- Exercise-7A-Workshop-ISO IMS-Ex-3Dokument2 SeitenExercise-7A-Workshop-ISO IMS-Ex-3jogender kumarNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- STUDY MANUAL Planning Your Career in Business (V3)Dokument56 SeitenSTUDY MANUAL Planning Your Career in Business (V3)Cristina IsbășescuNoch keine Bewertungen
- 2020 Greenhills Hostage Crisis Lea 3 ReportDokument4 Seiten2020 Greenhills Hostage Crisis Lea 3 ReportMary Grace PagurayanNoch keine Bewertungen
- D E F L H: Nurses in The PhilippinesDokument2 SeitenD E F L H: Nurses in The PhilippinesRyan Michael OducadoNoch keine Bewertungen
- Gautam Das Clinical ExaminationDokument233 SeitenGautam Das Clinical ExaminationHenry SugihartoNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Ebook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFDokument67 SeitenEbook Benzels Spine Surgery 2 Volume Set Techniques Complication Avoidance and Management PDF Full Chapter PDFgerald.wesolowski623100% (22)
- Physical Education and Health 12 - Q2 WEEK 7 8Dokument10 SeitenPhysical Education and Health 12 - Q2 WEEK 7 8Cristina Luz Cabana75% (4)
- Pros and Cons of Abortion To The Society Argumentative EssayDokument10 SeitenPros and Cons of Abortion To The Society Argumentative EssayimnasNoch keine Bewertungen
- Lifelong WellnessDokument3 SeitenLifelong Wellnessapi-404677881Noch keine Bewertungen
- MCQ 23Dokument10 SeitenMCQ 23Old driverNoch keine Bewertungen
- Posterior Fixation of APC-2 Pelvic Ring Injuries PDFDokument8 SeitenPosterior Fixation of APC-2 Pelvic Ring Injuries PDFgevowo3277Noch keine Bewertungen
- 4BI1 2B Que 20211116Dokument20 Seiten4BI1 2B Que 20211116Mo MisuratiNoch keine Bewertungen
- SDG Progress Report Special EditionDokument43 SeitenSDG Progress Report Special EditionSatya VNoch keine Bewertungen
- Reading Test 3Dokument10 SeitenReading Test 3Tuyết NhưNoch keine Bewertungen
- DLL Mod.1 Part 3 3RD QRTR G10Dokument7 SeitenDLL Mod.1 Part 3 3RD QRTR G10Kris Camille TanNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Masterkure-107 MsdsDokument2 SeitenMasterkure-107 MsdsNidDou100% (1)
- Cognitive Function Test (Executive Functioning)Dokument18 SeitenCognitive Function Test (Executive Functioning)stella kivuti0% (1)
- Assignment One Human DevelopmentDokument6 SeitenAssignment One Human DevelopmentjenNoch keine Bewertungen
- Predicting Teenage Girls' Sexual Activity and Contraception Use: An Application of Matching LawDokument16 SeitenPredicting Teenage Girls' Sexual Activity and Contraception Use: An Application of Matching LawPedro Pablo OchoaNoch keine Bewertungen
- Avery Hayden - How To Attract WomenDokument143 SeitenAvery Hayden - How To Attract WomenAng3l Ang3l100% (1)
- Title Disciplines of Social WorkDokument6 SeitenTitle Disciplines of Social WorkNicol Jay DuriguezNoch keine Bewertungen
- Womb As OasisDokument18 SeitenWomb As OasisMaria Paula SuarezNoch keine Bewertungen
- Instructions Ec120bDokument2 SeitenInstructions Ec120bAlejandro MamaniNoch keine Bewertungen
- STABILITY PROTOCOL - Revised (Sep21)Dokument2 SeitenSTABILITY PROTOCOL - Revised (Sep21)Ferdian Iwank IriyantoNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)