Das könnte Ihnen auch gefallen
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtVon EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtBewertung: 5 von 5 Sternen5/5 (1)
- AFib in ICUDokument11 SeitenAFib in ICUvarunNoch keine Bewertungen
- Cardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesVon EverandCardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesNoch keine Bewertungen
- Atrial Fibrillation in Congestive Heart Failure.Dokument13 SeitenAtrial Fibrillation in Congestive Heart Failure.Chau Khac ToanNoch keine Bewertungen
- Atrial Fibrillation (AF) : Myocardial Infarction or Pulmonary EmbolismDokument3 SeitenAtrial Fibrillation (AF) : Myocardial Infarction or Pulmonary EmbolismKurisu AadenNoch keine Bewertungen
- Articulo No. 17 Prevencion de ACV, Papel de AnticoagulacionDokument16 SeitenArticulo No. 17 Prevencion de ACV, Papel de AnticoagulacionNázareth DonisNoch keine Bewertungen
- Acute Decompensated Heart FailureDokument22 SeitenAcute Decompensated Heart Failurediomer123Noch keine Bewertungen
- Management of Atrial Fibrillation: ArrhythmiasDokument4 SeitenManagement of Atrial Fibrillation: ArrhythmiasHesbon MomanyiNoch keine Bewertungen
- Af JamaDokument10 SeitenAf JamaJose Evangelista RNoch keine Bewertungen
- Treatment of Atrial Fibrillation: Abhay Bajpai, Irina Savelieva, and A. John CammDokument20 SeitenTreatment of Atrial Fibrillation: Abhay Bajpai, Irina Savelieva, and A. John Cammbdalcin5512Noch keine Bewertungen
- AF KardiomiopatiDokument5 SeitenAF KardiomiopatiannisNoch keine Bewertungen
- 3390-Article Text-1555-3802-10-20200606Dokument12 Seiten3390-Article Text-1555-3802-10-20200606Mayara Bongestab ParteliNoch keine Bewertungen
- Right Heart Failure A Narrative Review For Emergency CliniciansDokument8 SeitenRight Heart Failure A Narrative Review For Emergency ClinicianssunhaolanNoch keine Bewertungen
- ADHF ManagementDokument6 SeitenADHF ManagementEsti YunitaNoch keine Bewertungen
- Acute Heart Failure Syndromes: Mihai Gheorghiade, MD, FACC, Peter S. Pang, MDDokument17 SeitenAcute Heart Failure Syndromes: Mihai Gheorghiade, MD, FACC, Peter S. Pang, MDcornelyNoch keine Bewertungen
- Atrial Fibrillation and Heart Failure - Cause or Effect?Dokument8 SeitenAtrial Fibrillation and Heart Failure - Cause or Effect?Cosmin GabrielNoch keine Bewertungen
- Atrial Fibrillation Occurring During Acute Hospitalization AHA 2023Dokument23 SeitenAtrial Fibrillation Occurring During Acute Hospitalization AHA 2023Lena Hinojosa SarabiaNoch keine Bewertungen
- Interesting ArticleDokument15 SeitenInteresting ArticleAnastasios TsarouchasNoch keine Bewertungen
- Acute Decompensated Heart Failure: ReviewDokument11 SeitenAcute Decompensated Heart Failure: ReviewFercee PrimulaNoch keine Bewertungen
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareDokument10 SeitenCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareMirachel AugustNoch keine Bewertungen
- Atrial FibrillationDokument18 SeitenAtrial FibrillationmamaluNoch keine Bewertungen
- 403 Full PDFDokument10 Seiten403 Full PDFKuroto YoshikiNoch keine Bewertungen
- Was Mer 2016Dokument6 SeitenWas Mer 2016Reinaldi octaNoch keine Bewertungen
- Pitfalls in The Evaluation of Shortness Breath - The ClinicsDokument19 SeitenPitfalls in The Evaluation of Shortness Breath - The ClinicsEdgardo Vargas AlvarezNoch keine Bewertungen
- 1.postoperative Arrhythmias After Cardiac SurgeryDokument16 Seiten1.postoperative Arrhythmias After Cardiac Surgeryganda gandaNoch keine Bewertungen
- Congestiveheartfailure: Michael C. Scott,, Michael E. WintersDokument10 SeitenCongestiveheartfailure: Michael C. Scott,, Michael E. WintersNicolás HonoresNoch keine Bewertungen
- HP Jul06 HeartDokument8 SeitenHP Jul06 HeartIlmi Dewi ANoch keine Bewertungen
- Fibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015Dokument11 SeitenFibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015alanRV12Noch keine Bewertungen
- Anti Coagulation in HFDokument7 SeitenAnti Coagulation in HFDina RyantiNoch keine Bewertungen
- Atrial Fibrillation - Annals of Internal Medicine (2023)Dokument18 SeitenAtrial Fibrillation - Annals of Internal Medicine (2023)silvermist100% (2)
- Acute Congestive Heart Failure in The Emergency DepartmentDokument9 SeitenAcute Congestive Heart Failure in The Emergency DepartmentAlanNoch keine Bewertungen
- Atrial Fibrillation: Diagnosis and TreatmentDokument8 SeitenAtrial Fibrillation: Diagnosis and TreatmentCut Thalya Alissya RahmaNoch keine Bewertungen
- Oncologic Mechanical Emergencies 2014 Emergency Medicine Clinics of North AmericaDokument14 SeitenOncologic Mechanical Emergencies 2014 Emergency Medicine Clinics of North AmericamarcosjuniormutucaNoch keine Bewertungen
- Fa Muy NuevoDokument8 SeitenFa Muy NuevoJoshua Alberto Gracia MancillaNoch keine Bewertungen
- Articulo COVID 19Dokument9 SeitenArticulo COVID 19Omaira TovarNoch keine Bewertungen
- Overview of Nurses' Role in Management of Patient With Atrial FibrillationDokument5 SeitenOverview of Nurses' Role in Management of Patient With Atrial FibrillationAhmed AlkhaqaniNoch keine Bewertungen
- Congestive Heart Failure/Pulmonary Edema Case FileDokument4 SeitenCongestive Heart Failure/Pulmonary Edema Case Filehttps://medical-phd.blogspot.comNoch keine Bewertungen
- Chronic Atrial Fibrillation - Highlights & BasicsDokument5 SeitenChronic Atrial Fibrillation - Highlights & BasicsRishabh SharmaNoch keine Bewertungen
- Fi ADokument67 SeitenFi AalfonsoNoch keine Bewertungen
- Atrial FibrillationDokument60 SeitenAtrial FibrillationNurul ImaniarNoch keine Bewertungen
- Nihms 840977Dokument28 SeitenNihms 840977adinda.larastitiNoch keine Bewertungen
- Bader Madoukh, Ayman Battisha, Henry Ukwu, Mohammed Al-Sadawi, Shakil ShaikhDokument4 SeitenBader Madoukh, Ayman Battisha, Henry Ukwu, Mohammed Al-Sadawi, Shakil ShaikhputriayuratnasariNoch keine Bewertungen
- Fa JamaDokument11 SeitenFa JamaFrancis MaldonadoNoch keine Bewertungen
- Congestive Heart FailureDokument16 SeitenCongestive Heart FailureRahmat Burhanudin RamdaniNoch keine Bewertungen
- Accepted Manuscript: 10.1016/j.chest.2018.03.040Dokument27 SeitenAccepted Manuscript: 10.1016/j.chest.2018.03.040Patty MArivel ReinosoNoch keine Bewertungen
- Heart FailureDokument4 SeitenHeart FailureHany ElbarougyNoch keine Bewertungen
- Acute Heart Failure SyndromesDokument19 SeitenAcute Heart Failure SyndromesLiz EscuetaNoch keine Bewertungen
- Oncologicmechanical Emergencies: Umar A. Khan,, Carl B. Shanholtz,, Michael T. MccurdyDokument14 SeitenOncologicmechanical Emergencies: Umar A. Khan,, Carl B. Shanholtz,, Michael T. MccurdySandra PargaNoch keine Bewertungen
- Advances Management ADHFDokument14 SeitenAdvances Management ADHFAnonymous NeRC5JYiSNoch keine Bewertungen
- Syncope - Electrocardiographic and Clinical CorrelationDokument16 SeitenSyncope - Electrocardiographic and Clinical CorrelationNANDY LUZ FERIA DIAZNoch keine Bewertungen
- Why Does Atrial Fibrillation Occur?Dokument38 SeitenWhy Does Atrial Fibrillation Occur?khansa nabilaNoch keine Bewertungen
- Referat Dysfunction Diastolic and Implication in AnathesiaDokument32 SeitenReferat Dysfunction Diastolic and Implication in AnathesiaRia Raissa FalaNoch keine Bewertungen
- 428 FullDokument12 Seiten428 FullAyesha PeerNoch keine Bewertungen
- Chronic Arrhythmia ManagementDokument44 SeitenChronic Arrhythmia ManagementSulaiman TahsinNoch keine Bewertungen
- Atrial Fibrilation and Stroke PreventionDokument2 SeitenAtrial Fibrilation and Stroke PreventionAnnisa SyaflianiNoch keine Bewertungen
- Mechanismsofstrokeinatrial Fibrillation: Jose Maria Castellano,, Jason Chinitz,, Jonathan Willner,, Valentin FusterDokument11 SeitenMechanismsofstrokeinatrial Fibrillation: Jose Maria Castellano,, Jason Chinitz,, Jonathan Willner,, Valentin FusterCamilo GomezNoch keine Bewertungen
- Acute Heart Failure Syndromes: Kelompok CDokument29 SeitenAcute Heart Failure Syndromes: Kelompok CErwin BawonoNoch keine Bewertungen
- Chronic Heart Failure-Part IDokument18 SeitenChronic Heart Failure-Part IdrtpkNoch keine Bewertungen
- Approach To Cardiac PatientDokument6 SeitenApproach To Cardiac PatientDemuel Dee L. BertoNoch keine Bewertungen
- Trends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzDokument9 SeitenTrends in Cardiovascular Medicine: Lauren Sinnenberg, Michael M. GivertzJulio PorrasNoch keine Bewertungen
- 2015 Article 52Dokument10 Seiten2015 Article 52Attilio Del RossoNoch keine Bewertungen
- Atrial Fibrillation in Athletes: A Lesson in The Virtue of ModerationDokument8 SeitenAtrial Fibrillation in Athletes: A Lesson in The Virtue of ModerationAttilio Del RossoNoch keine Bewertungen
- CENTURIA II - FAQ & ERRATA - PDF Download GratuitoDokument2 SeitenCENTURIA II - FAQ & ERRATA - PDF Download GratuitoAttilio Del RossoNoch keine Bewertungen
- How To Perform A Transseptal Puncture: Mark J EarleyDokument9 SeitenHow To Perform A Transseptal Puncture: Mark J EarleyAttilio Del RossoNoch keine Bewertungen
- Esercizio e Fa 2Dokument8 SeitenEsercizio e Fa 2Attilio Del RossoNoch keine Bewertungen
- Cardioversion of Atrial Fibrillation in Obese Patients: Results From The Cardioversion-BMI Randomized Controlled TrialDokument22 SeitenCardioversion of Atrial Fibrillation in Obese Patients: Results From The Cardioversion-BMI Randomized Controlled TrialAttilio Del RossoNoch keine Bewertungen
- EmergencymanagmentDokument9 SeitenEmergencymanagmentAttilio Del RossoNoch keine Bewertungen
- The Pulmonary Artery Catheter: Is It Still Alive?: ReviewDokument5 SeitenThe Pulmonary Artery Catheter: Is It Still Alive?: ReviewAttilio Del RossoNoch keine Bewertungen
- What Is The Optimum Method of Weaning Intra-Aortic Balloon Pumps?Dokument4 SeitenWhat Is The Optimum Method of Weaning Intra-Aortic Balloon Pumps?Attilio Del RossoNoch keine Bewertungen
- Prevention of Embolization Prior To and After Restoration of Sinus Rhythm in Atrial Fibrillation - UpToDateDokument25 SeitenPrevention of Embolization Prior To and After Restoration of Sinus Rhythm in Atrial Fibrillation - UpToDateAttilio Del RossoNoch keine Bewertungen
- Meccanical SupportDokument19 SeitenMeccanical SupportAttilio Del RossoNoch keine Bewertungen
- Guidelines On The Management of Atrial Fibrillation in The Emergency Department: A Critical AppraisalDokument11 SeitenGuidelines On The Management of Atrial Fibrillation in The Emergency Department: A Critical AppraisalAttilio Del RossoNoch keine Bewertungen
- Come Monitorare? Dallo Swan Ganz Al Pulse Contour.: Alessandro LocatelliDokument47 SeitenCome Monitorare? Dallo Swan Ganz Al Pulse Contour.: Alessandro LocatelliAttilio Del RossoNoch keine Bewertungen
- Door To Unload: A New Paradigm For The Management of Cardiogenic ShockDokument8 SeitenDoor To Unload: A New Paradigm For The Management of Cardiogenic ShockAttilio Del RossoNoch keine Bewertungen
- Obituary: Pulmonary Artery Catheter 1970 To 2013: Review Open AccessDokument6 SeitenObituary: Pulmonary Artery Catheter 1970 To 2013: Review Open AccessAttilio Del RossoNoch keine Bewertungen
- Rapida FireDokument14 SeitenRapida FireAttilio Del RossoNoch keine Bewertungen
- Cardiogenic ShockDokument5 SeitenCardiogenic ShockAttilio Del RossoNoch keine Bewertungen
- Hemodymamic MonitoringDokument14 SeitenHemodymamic MonitoringAttilio Del RossoNoch keine Bewertungen
- Trench Grand HommeDokument11 SeitenTrench Grand HommeAttilio Del RossoNoch keine Bewertungen
- Migration of An Injectable' Loop Recorder in The Dorsal Pleural CavityDokument1 SeiteMigration of An Injectable' Loop Recorder in The Dorsal Pleural CavityAttilio Del RossoNoch keine Bewertungen
- BS Company RecordsDokument2 SeitenBS Company RecordstNoch keine Bewertungen
- Marketing Research ProjectDokument37 SeitenMarketing Research ProjectVijay100% (15)
- Sworn Statement of Assets, Liabilities and Net WorthDokument2 SeitenSworn Statement of Assets, Liabilities and Net WorthFaidah Palawan AlawiNoch keine Bewertungen
- Packing Shipping InstructionsDokument2 SeitenPacking Shipping InstructionsJ.V. Siritt ChangNoch keine Bewertungen
- Facility Management SystemDokument6 SeitenFacility Management Systemshah007zaad100% (1)
- Define Constitution. What Is The Importance of Constitution in A State?Dokument2 SeitenDefine Constitution. What Is The Importance of Constitution in A State?Carmela AlfonsoNoch keine Bewertungen
- ACCOUNTS Foundation Paper1Dokument336 SeitenACCOUNTS Foundation Paper1mukni613324100% (1)
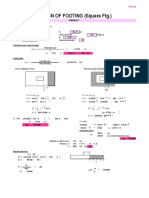
- Design of Footing (Square FTG.) : M Say, L 3.75Dokument2 SeitenDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNoch keine Bewertungen
- Installing Oracle Fail SafeDokument14 SeitenInstalling Oracle Fail SafeSantiago ArgibayNoch keine Bewertungen
- BCCA Semester New Syllabus Direction 2016-17 PDFDokument76 SeitenBCCA Semester New Syllabus Direction 2016-17 PDFChetana Gorakh100% (1)
- Report - Fostering The Railway Sector Through The European Green Deal PDFDokument43 SeitenReport - Fostering The Railway Sector Through The European Green Deal PDFÁdámHegyiNoch keine Bewertungen
- Addendum No.1: Indianapolis Metropolitan Airport T-Hangar Taxilane Rehabilitation IAA Project No. M-12-032Dokument22 SeitenAddendum No.1: Indianapolis Metropolitan Airport T-Hangar Taxilane Rehabilitation IAA Project No. M-12-032stretch317Noch keine Bewertungen
- Republic vs. CA (G.R. No. 139592, October 5, 2000)Dokument11 SeitenRepublic vs. CA (G.R. No. 139592, October 5, 2000)Alexandra Mae GenorgaNoch keine Bewertungen
- RH S65A SSVR Users ManualDokument11 SeitenRH S65A SSVR Users ManualMohd Fauzi YusohNoch keine Bewertungen
- EquisetopsidaDokument4 SeitenEquisetopsidax456456456xNoch keine Bewertungen
- Event Management (MAX FIT)Dokument12 SeitenEvent Management (MAX FIT)vkrish6Noch keine Bewertungen
- BS351: Financial Reporting: Learning ObjectivesDokument3 SeitenBS351: Financial Reporting: Learning ObjectivesMajeed Ullah KhanNoch keine Bewertungen
- TDS - Total - Carter 68 - Wyh - 202201 - en - IdnDokument1 SeiteTDS - Total - Carter 68 - Wyh - 202201 - en - IdnAnya J PamungkasNoch keine Bewertungen
- 40 MTCNA QuestionsDokument10 Seiten40 MTCNA QuestionsM Aris Firjatullah FirdausNoch keine Bewertungen
- Moeller Vol07 - Tab02 Signal Tower PDFDokument46 SeitenMoeller Vol07 - Tab02 Signal Tower PDFArga WahyumiantoNoch keine Bewertungen
- Gears, Splines, and Serrations: Unit 24Dokument8 SeitenGears, Splines, and Serrations: Unit 24Satish Dhandole100% (1)
- CS 252: Computer Organization and Architecture II: Lecture 5 - The Memory SystemDokument29 SeitenCS 252: Computer Organization and Architecture II: Lecture 5 - The Memory SystemJonnahNoch keine Bewertungen
- Automatic Star Delta StarterDokument11 SeitenAutomatic Star Delta StarterAmg 360Noch keine Bewertungen
- Dinner Theater Business PlanDokument21 SeitenDinner Theater Business PlanBhumika KariaNoch keine Bewertungen
- Leadership and Decision Making PDFDokument34 SeitenLeadership and Decision Making PDFNhi PhamNoch keine Bewertungen
- Determination of The Amount of Hardness in Water Using Soap SolutionDokument3 SeitenDetermination of The Amount of Hardness in Water Using Soap SolutionlokeshjoshimjNoch keine Bewertungen
- Np2 AnswerDokument13 SeitenNp2 AnswerMarie Jhoana100% (1)
- Midterm Quiz 1 March 9.2021 QDokument5 SeitenMidterm Quiz 1 March 9.2021 QThalia RodriguezNoch keine Bewertungen
- TCRP Wheel Rail Noise ReportDokument220 SeitenTCRP Wheel Rail Noise ReportAnonymous OmwbxkB100% (1)
- 10.isca RJCS 2015 106Dokument5 Seiten10.isca RJCS 2015 106Touhid IslamNoch keine Bewertungen