Das könnte Ihnen auch gefallen
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesVon EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNoch keine Bewertungen
- Ni Hms 935657Dokument15 SeitenNi Hms 935657AHMAD FUDHAIL AHMAD ZAKINoch keine Bewertungen
- Radiol 221894Dokument10 SeitenRadiol 221894JEFFERSON MUÑOZNoch keine Bewertungen
- Developing Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019Dokument8 SeitenDeveloping Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019AbhishekNoch keine Bewertungen
- Clinical Diagnosis of Uncomplicated, Acute Appendicitis Remains An Imperfect ScienceDokument3 SeitenClinical Diagnosis of Uncomplicated, Acute Appendicitis Remains An Imperfect ScienceHector ReinozoNoch keine Bewertungen
- 08 Can We Safely Apply The Ottawa Ankle Rules To ChildrenDokument3 Seiten08 Can We Safely Apply The Ottawa Ankle Rules To ChildrenAlejandro Godoy SaidNoch keine Bewertungen
- Teitcher 2022 Ic 220142 1657735397.32063Dokument3 SeitenTeitcher 2022 Ic 220142 1657735397.32063Orlin ZlatarskiNoch keine Bewertungen
- IRB Proposal - PSU Aorta NLP ProjectDokument39 SeitenIRB Proposal - PSU Aorta NLP Projectjhk0428Noch keine Bewertungen
- Predicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDokument9 SeitenPredicting Surgical Complications in Patients Undergoing Elective Adult Spinal Deformity Procedures Using Machine LearningDr-Rabia AlmamalookNoch keine Bewertungen
- Radiation Exposure and Cost Influence Physician Medical Image Decision MakingDokument5 SeitenRadiation Exposure and Cost Influence Physician Medical Image Decision Makingكن صديقيNoch keine Bewertungen
- Respirology - 2019 - Lovejoy - Application of Artificial Intelligence in Respiratory Medicine Has The Time ArrivedDokument2 SeitenRespirology - 2019 - Lovejoy - Application of Artificial Intelligence in Respiratory Medicine Has The Time Arrivedchristopher.lovejoy1Noch keine Bewertungen
- PIIS2589750020301606Dokument3 SeitenPIIS2589750020301606Sadaf QasimNoch keine Bewertungen
- 14.Osteo PredictionDokument9 Seiten14.Osteo Predictionraja.m2023Noch keine Bewertungen
- Dose Differences Due To Variance in Contours of The Optic ChiasmDokument15 SeitenDose Differences Due To Variance in Contours of The Optic Chiasmapi-527662950Noch keine Bewertungen
- Journal Pone 0247330Dokument14 SeitenJournal Pone 0247330viju001Noch keine Bewertungen
- Skeletal Development of The Hand and Wrist Digital PDFDokument9 SeitenSkeletal Development of The Hand and Wrist Digital PDFangie catalina estupiñan mirandaNoch keine Bewertungen
- Lung Tumor Localization and Visualization in ChestDokument17 SeitenLung Tumor Localization and Visualization in ChestAida Fitriyane HamdaniNoch keine Bewertungen
- Detrano 1989Dokument7 SeitenDetrano 1989Lilims LilithNoch keine Bewertungen
- Rcsann 2016 0048Dokument6 SeitenRcsann 2016 0048fabian arassiNoch keine Bewertungen
- The Reliability of Convolution Neural Networks Diagnosing Malignancy in MammographyDokument3 SeitenThe Reliability of Convolution Neural Networks Diagnosing Malignancy in Mammographyapi-436279390Noch keine Bewertungen
- C - SpineDokument10 SeitenC - SpineCharly MontielNoch keine Bewertungen
- Thursday, October 10, 2013 4:10 - 5:10 Concurrent Session: TraumaDokument2 SeitenThursday, October 10, 2013 4:10 - 5:10 Concurrent Session: TraumaPeko PekoNoch keine Bewertungen
- Triage tools for detecting cervical spine injury in paediatric trauma patients -Dokument41 SeitenTriage tools for detecting cervical spine injury in paediatric trauma patients -d69hffy472Noch keine Bewertungen
- Artificial Intelligence - INFORMSDokument5 SeitenArtificial Intelligence - INFORMSMiguel GarcíaNoch keine Bewertungen
- Jurnal Diagnostik ADokument8 SeitenJurnal Diagnostik AImtina AhdaNoch keine Bewertungen
- Disease Prediction Using Machine Learning Algorithms KNN and CNNDokument7 SeitenDisease Prediction Using Machine Learning Algorithms KNN and CNNIJRASETPublications100% (1)
- Use of Ultrasonography As A Diagnostic and Therapeutic ToolDokument11 SeitenUse of Ultrasonography As A Diagnostic and Therapeutic ToolVojtěch ŠmídNoch keine Bewertungen
- Scientific Abstracts Friday, 14 June 2019 1015Dokument1 SeiteScientific Abstracts Friday, 14 June 2019 1015حسام الدين إسماعيلNoch keine Bewertungen
- Roils Case StudyDokument3 SeitenRoils Case Studyapi-483339757Noch keine Bewertungen
- Clinical Trials in BrainDokument16 SeitenClinical Trials in Brainmadhukar1978Noch keine Bewertungen
- Performance of A Novel Risk Model For Deep Sternal Wound Infection After Coronary Artery Bypass GraftingDokument8 SeitenPerformance of A Novel Risk Model For Deep Sternal Wound Infection After Coronary Artery Bypass GraftingMartha CeciliaNoch keine Bewertungen
- Langer Hui Zen 2019Dokument10 SeitenLanger Hui Zen 2019Marco Morillo RodríguezNoch keine Bewertungen
- Deepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningDokument10 SeitenDeepaaa: Clinically Applicable and Generalizable Detection of Abdominal Aortic Aneurysm Using Deep LearningIzzHyukNoch keine Bewertungen
- Thyroid ReportDokument28 SeitenThyroid ReportLouis OdhiamboNoch keine Bewertungen
- Article 5Dokument10 SeitenArticle 5Tashu SardaNoch keine Bewertungen
- Cells 12 01847Dokument14 SeitenCells 12 01847yongkyNoch keine Bewertungen
- Jurnal 5Dokument5 SeitenJurnal 5Devita SanangkaNoch keine Bewertungen
- Convolutional Neural Network For Automated FLAIR Lesion Segmentation On Clinical Brain MR ImagingDokument9 SeitenConvolutional Neural Network For Automated FLAIR Lesion Segmentation On Clinical Brain MR ImagingTigabu YayaNoch keine Bewertungen
- International Journal of Health Sciences and ResearchDokument7 SeitenInternational Journal of Health Sciences and Researchrhegi isdiara FairuzNoch keine Bewertungen
- Of March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DDokument9 SeitenOf March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DAhana MukherjeeNoch keine Bewertungen
- First Page PDFDokument1 SeiteFirst Page PDFAnonymous 0vDTRVnNoch keine Bewertungen
- Xi, 2021 Tumor Associated Collagen SignaturesDokument15 SeitenXi, 2021 Tumor Associated Collagen Signaturesevahendrickx03Noch keine Bewertungen
- Radiol 2020190283Dokument12 SeitenRadiol 2020190283Raghavendran T BNoch keine Bewertungen
- Shti247 0386Dokument5 SeitenShti247 0386Hema Latha Krishna NairNoch keine Bewertungen
- BMJ f7095Dokument9 SeitenBMJ f7095Luis Gerardo Pérez CastroNoch keine Bewertungen
- Trauma Clinical Guideline 2017Dokument7 SeitenTrauma Clinical Guideline 2017Paolo ContrerasNoch keine Bewertungen
- A Detection and Segmentation of Medical Image Using Machine Learning AlgorithmsDokument5 SeitenA Detection and Segmentation of Medical Image Using Machine Learning AlgorithmsNazmul HassanNoch keine Bewertungen
- Two Decades of Hand TransplantationDokument10 SeitenTwo Decades of Hand TransplantationTamsin Athalie NicholsonNoch keine Bewertungen
- ECR 2022 ProgrammeDokument1.126 SeitenECR 2022 ProgrammejbmbritoNoch keine Bewertungen
- Editorial: Artificial Intelligence in Medical ApplicationsDokument3 SeitenEditorial: Artificial Intelligence in Medical Applicationsabelteshe_340263389Noch keine Bewertungen
- Predicting 3D Body Shape and Body Composition From Conventional 2D PhotographyDokument29 SeitenPredicting 3D Body Shape and Body Composition From Conventional 2D PhotographyGaltieri OtavioNoch keine Bewertungen
- Marcadores de AlzheimerDokument10 SeitenMarcadores de AlzheimerAna Luzia NassifNoch keine Bewertungen
- 551Dokument7 Seiten551dilkulNoch keine Bewertungen
- AR6TIFICIALDokument9 SeitenAR6TIFICIALutip25Noch keine Bewertungen
- PRedice CV Mortality With CT Nat Comm 2021Dokument9 SeitenPRedice CV Mortality With CT Nat Comm 2021Guilherme Taborda RibasNoch keine Bewertungen
- Cystic Lesions of The Pituitary Clinicopathological Features Distinguishing Craniopharyngioma, Rathke - S Cleft Cyst, and Arachnoid Cyst, 1999Dokument11 SeitenCystic Lesions of The Pituitary Clinicopathological Features Distinguishing Craniopharyngioma, Rathke - S Cleft Cyst, and Arachnoid Cyst, 1999CAMILO ARMANDO BENAVIDES BURBANONoch keine Bewertungen
- Good 2 Accuracy - of - The - Defining - CharaDokument9 SeitenGood 2 Accuracy - of - The - Defining - CharaAhmad Umar MukhtarNoch keine Bewertungen
- Poster Viewing I Tuesday 1 May 2018 Iii75Dokument2 SeitenPoster Viewing I Tuesday 1 May 2018 Iii75Firdaus Septhy ArdhyanNoch keine Bewertungen
- Jassal Et Al. - 2023 - Artificial Intelligence For Pre-Operative DiagnosisDokument10 SeitenJassal Et Al. - 2023 - Artificial Intelligence For Pre-Operative DiagnosisJamesLeeNoch keine Bewertungen
- Ultrasound Imaging ThesisDokument7 SeitenUltrasound Imaging Thesisbrendazerrindependence100% (2)
- Improving Fairness in Machine Learning Systems: What Do Industry Practitioners Need?Dokument13 SeitenImproving Fairness in Machine Learning Systems: What Do Industry Practitioners Need?ChrisNoch keine Bewertungen
- Brinkman2019 Article AndreasVesalius1515-1564OnAnimDokument8 SeitenBrinkman2019 Article AndreasVesalius1515-1564OnAnimChrisNoch keine Bewertungen
- Safe But Lonely? Loneliness, Anxiety, and Depression Symptoms and COVID-19Dokument11 SeitenSafe But Lonely? Loneliness, Anxiety, and Depression Symptoms and COVID-19ChrisNoch keine Bewertungen
- Searching For Collective Behavior in A Small BrainDokument14 SeitenSearching For Collective Behavior in A Small BrainChrisNoch keine Bewertungen
- The Hopkins Verbal Learning Test An in Depth Analysis of Recall PatternsDokument22 SeitenThe Hopkins Verbal Learning Test An in Depth Analysis of Recall PatternsChrisNoch keine Bewertungen
- 1 3 PDFDokument7 Seiten1 3 PDFChrisNoch keine Bewertungen
- 522 FullDokument5 Seiten522 FullChrisNoch keine Bewertungen
- Deep Reinforcement Learning: An OverviewDokument150 SeitenDeep Reinforcement Learning: An OverviewOscar Julian Perdomo CharryNoch keine Bewertungen
- Współczesne Tabu Językowe, Czyli O Czym Nie Mówią Polacy: March 2019Dokument24 SeitenWspółczesne Tabu Językowe, Czyli O Czym Nie Mówią Polacy: March 2019ChrisNoch keine Bewertungen
- Young2019 Article OlfactoryImageryIsExactlyWhatIDokument25 SeitenYoung2019 Article OlfactoryImageryIsExactlyWhatIChrisNoch keine Bewertungen
- Beker 2020 Oi 200010Dokument16 SeitenBeker 2020 Oi 200010ChrisNoch keine Bewertungen
- Lesson 1 Writing ClearlyDokument16 SeitenLesson 1 Writing ClearlyChrisNoch keine Bewertungen
- Taylor, Wang, Kaiser - 2017Dokument9 SeitenTaylor, Wang, Kaiser - 2017ChrisNoch keine Bewertungen
- Fischl02 LabelingDokument15 SeitenFischl02 LabelingChrisNoch keine Bewertungen
- Word Prevalence Norms For 62K English Lemmas FinalDokument29 SeitenWord Prevalence Norms For 62K English Lemmas FinalChrisNoch keine Bewertungen
- Yjbm 92 1 37 PDFDokument15 SeitenYjbm 92 1 37 PDFChrisNoch keine Bewertungen
- 22 New Hardware For Massive Neural NetworksDokument10 Seiten22 New Hardware For Massive Neural NetworksChrisNoch keine Bewertungen
- IQ, OQ, PQ: A Quick Guide To Process ValidationDokument9 SeitenIQ, OQ, PQ: A Quick Guide To Process ValidationGonzalo MazaNoch keine Bewertungen
- Ice-Cream ProductionDokument65 SeitenIce-Cream ProductionMujtaba HaseebNoch keine Bewertungen
- Appendix 1c Bridge Profiles Allan TrussesDokument43 SeitenAppendix 1c Bridge Profiles Allan TrussesJosue LewandowskiNoch keine Bewertungen
- Usg Sheetrock® Brand Acoustical SealantDokument3 SeitenUsg Sheetrock® Brand Acoustical SealantHoracio PadillaNoch keine Bewertungen
- Essential Guide VLSI Aspirants FAQ Physical DesignDokument3 SeitenEssential Guide VLSI Aspirants FAQ Physical DesignRohith RajNoch keine Bewertungen
- High Level Cyber Security Assessment - Detailed ReportDokument57 SeitenHigh Level Cyber Security Assessment - Detailed Reportdobie_e_martinNoch keine Bewertungen
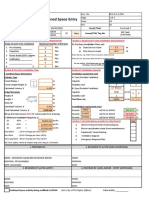
- Ventilation Plan For Confined Space EntryDokument9 SeitenVentilation Plan For Confined Space EntryMohamad Nazmi Mohamad Rafian100% (1)
- Pengaruh Komunikasi DGN KinerjaDokument15 SeitenPengaruh Komunikasi DGN KinerjaTitHa AwallunnisaNoch keine Bewertungen
- GIYA Classroom VisitationDokument4 SeitenGIYA Classroom VisitationRussell Moralla100% (2)
- Porter's Five Forces: Submitted by Subham Chakraborty PGDMDokument5 SeitenPorter's Five Forces: Submitted by Subham Chakraborty PGDMSubham ChakrabortyNoch keine Bewertungen
- Communication Systems Engineering John G Proakis Masoud Salehi PDFDokument2 SeitenCommunication Systems Engineering John G Proakis Masoud Salehi PDFKatie0% (2)
- 3D Printing Seminar REPORT-srijanDokument26 Seiten3D Printing Seminar REPORT-srijanSrijan UpadhyayNoch keine Bewertungen
- Win Top Prizes in Investizo's SuperTrader ContestDokument3 SeitenWin Top Prizes in Investizo's SuperTrader ContestJafrid NassifNoch keine Bewertungen
- Project 4 FinalDokument2 SeitenProject 4 Finalapi-307253935Noch keine Bewertungen
- Phy433 Lab Report 1Dokument9 SeitenPhy433 Lab Report 1rabbani abdul rahimNoch keine Bewertungen
- GRADES 1 To 12 Daily Lesson Log Monday Tuesday Wednesday Thursday FridayDokument3 SeitenGRADES 1 To 12 Daily Lesson Log Monday Tuesday Wednesday Thursday FridaySheilaMarB.Esteban100% (1)
- Mathematics 10 Performance Task 1Dokument2 SeitenMathematics 10 Performance Task 1SnowNoch keine Bewertungen
- Piccolo: Operating and Maintenance Instructions For The Deck OvenDokument44 SeitenPiccolo: Operating and Maintenance Instructions For The Deck OvenAdam B100% (1)
- Dinosaur Bones - American Museum of Natural HistoryDokument7 SeitenDinosaur Bones - American Museum of Natural HistoryNicholas FeatherstonNoch keine Bewertungen
- Elon Musk: AI Is A Fundamental Risk To The Existence of Human CivilizationDokument19 SeitenElon Musk: AI Is A Fundamental Risk To The Existence of Human CivilizationBDApp StarNoch keine Bewertungen
- Earthquake Faults and Tectonic Plate Boundaries ExplainedDokument21 SeitenEarthquake Faults and Tectonic Plate Boundaries ExplainedAngelo RemeticadoNoch keine Bewertungen
- Sany - SCC8300 Crawler CraneDokument52 SeitenSany - SCC8300 Crawler CraneNunoNoch keine Bewertungen
- Maths ReportDokument3 SeitenMaths ReportShishir BogatiNoch keine Bewertungen
- VSP BrochureDokument33 SeitenVSP BrochuresudhakarrrrrrNoch keine Bewertungen
- Purchase OrderDokument2 SeitenPurchase OrderNicole LomasangNoch keine Bewertungen
- The Danieli Danarc Plus M Furnace at Abs Meltshop: Aldo A. Fior Danieli C M - Process Engineer Buttrio, ItalyDokument6 SeitenThe Danieli Danarc Plus M Furnace at Abs Meltshop: Aldo A. Fior Danieli C M - Process Engineer Buttrio, ItalyBrandon CoxNoch keine Bewertungen
- Snel White Paper 2020Dokument18 SeitenSnel White Paper 2020Zgodan NezgodanNoch keine Bewertungen
- Features Description: LT3598 6-String 30ma LED Driver With 1.5% Current MatchingDokument24 SeitenFeatures Description: LT3598 6-String 30ma LED Driver With 1.5% Current MatchingMick Thomson RcNoch keine Bewertungen
- Research Associate in The DFG Graduate Program - Collective Decision-Making - (12 Positions) - 28 Subsection 3 HMBHGDokument3 SeitenResearch Associate in The DFG Graduate Program - Collective Decision-Making - (12 Positions) - 28 Subsection 3 HMBHGFiya ShahNoch keine Bewertungen
- Adv - Student - HandbookDokument61 SeitenAdv - Student - HandbookOmkar BezzankiNoch keine Bewertungen