Das könnte Ihnen auch gefallen
- Fluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceVon EverandFluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceBewertung: 5 von 5 Sternen5/5 (2)
- Bio Disc IntroDokument19 SeitenBio Disc IntroBrako Jones100% (1)
- The Water Prescription: For Health, Vitality, and RejuvenationVon EverandThe Water Prescription: For Health, Vitality, and RejuvenationBewertung: 5 von 5 Sternen5/5 (2)
- The Body Remembers Volume 2: Revolutionizing Trauma Treatment - Babette RothschildDokument6 SeitenThe Body Remembers Volume 2: Revolutionizing Trauma Treatment - Babette Rothschildnamonomi0% (4)
- Output IN ChemistryDokument11 SeitenOutput IN ChemistryMay Pavia100% (1)
- ACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idDokument14 SeitenACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idCenitserNoch keine Bewertungen
- Nursing Fluids and ElectrolytesDokument14 SeitenNursing Fluids and Electrolytesaga1028100% (18)
- Save Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced World: How to Save Your LifeVon EverandSave Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced World: How to Save Your LifeBewertung: 2 von 5 Sternen2/5 (2)
- Anatomical TermsDokument38 SeitenAnatomical Termsrajni singhNoch keine Bewertungen
- LevothyroxineDokument5 SeitenLevothyroxineJackieMaeNoch keine Bewertungen
- Fluid and Electrolyte 2018-1Dokument33 SeitenFluid and Electrolyte 2018-1EN.BASSAM ALSABAHI100% (1)
- Reviewer Chapter 52 FluidsDokument8 SeitenReviewer Chapter 52 FluidsKeren GaciasNoch keine Bewertungen
- IV Fluids (What Nurses Need To Know)Dokument9 SeitenIV Fluids (What Nurses Need To Know)ChelseaLovell100% (2)
- Fluid and ElyctrolyteDokument49 SeitenFluid and Elyctrolyteuuuhbnb lplhghNoch keine Bewertungen
- A Study of Alkaline Ionized Water: Educational ManualDokument15 SeitenA Study of Alkaline Ionized Water: Educational ManualJohan Korthout100% (1)
- Unit 3 Fluid and ElectrolyteDokument20 SeitenUnit 3 Fluid and ElectrolyteChandan ShahNoch keine Bewertungen
- Fluid, Electrolyte, and Acid-Base BalanceDokument41 SeitenFluid, Electrolyte, and Acid-Base BalanceRn nadeenNoch keine Bewertungen
- Fluid and ElyctrolyteDokument49 SeitenFluid and Elyctrolyteuuuhbnb lplhgh100% (2)
- Georg Lukács The Process of Democratization 1968 PDFDokument191 SeitenGeorg Lukács The Process of Democratization 1968 PDFmusawar420Noch keine Bewertungen
- Understanding IV FluidsDokument2 SeitenUnderstanding IV FluidsJoe Anne Maniulit, MSN, RN100% (5)
- Lymph Health: The Key to a Strong Immune SystemVon EverandLymph Health: The Key to a Strong Immune SystemBewertung: 5 von 5 Sternen5/5 (1)
- The Magic MountainDokument3 SeitenThe Magic MountainKyla Claire BiñasNoch keine Bewertungen
- Save Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced WorldVon EverandSave Your Life with the Elixir of Water: Becoming pH Balanced in an Unbalanced WorldNoch keine Bewertungen
- Water Pollution ControlVon EverandWater Pollution ControlSuresh T. NesaratnamNoch keine Bewertungen
- Pulpectomy ProceduresDokument3 SeitenPulpectomy ProceduresITS DENTAL COLLEGE Greater NoidaNoch keine Bewertungen
- Name - Suraj Sala-WPS OfficeDokument7 SeitenName - Suraj Sala-WPS OfficeMariam UmarNoch keine Bewertungen
- Water As An Essential Nutrient The PhysiologyDokument10 SeitenWater As An Essential Nutrient The PhysiologyGianinaMihalacheCojocaruNoch keine Bewertungen
- Body Fluids and BloodDokument83 SeitenBody Fluids and Bloodalthea jade villadongaNoch keine Bewertungen
- PhysiologyDokument84 SeitenPhysiologyWilliam BufNoch keine Bewertungen
- Fluid and Electrolyte Homeostasis: Facts Based Comprehensive StudyDokument5 SeitenFluid and Electrolyte Homeostasis: Facts Based Comprehensive StudyAchmat riyadiNoch keine Bewertungen
- WaterDokument6 SeitenWaterSwaichchha BasnetNoch keine Bewertungen
- Water Physiology Essentiality, Metabolism, And.8Dokument6 SeitenWater Physiology Essentiality, Metabolism, And.8Patricia ChirinosNoch keine Bewertungen
- Lecture 14. Water - Mineral Metabolism. Biochemistry of Kidneys and UrineDokument39 SeitenLecture 14. Water - Mineral Metabolism. Biochemistry of Kidneys and UrineВіталій Михайлович НечипорукNoch keine Bewertungen
- Benefits of Water For HealthDokument3 SeitenBenefits of Water For HealthJesus TerrazasNoch keine Bewertungen
- Gen Bio 2 Q4 Week 4 and 5Dokument7 SeitenGen Bio 2 Q4 Week 4 and 5Ginno OsmilloNoch keine Bewertungen
- Water and Electrolyte BalanceDokument11 SeitenWater and Electrolyte BalanceVincent Maralit MaterialNoch keine Bewertungen
- Fluids Electrolytes 1Dokument43 SeitenFluids Electrolytes 1QueenClerk VillarteNoch keine Bewertungen
- Body and Electrolyte BalanceDokument6 SeitenBody and Electrolyte BalanceCK SinghNoch keine Bewertungen
- PGDBC IDokument47 SeitenPGDBC IDr Estari MamidalaNoch keine Bewertungen
- Anaphy EmanualDokument12 SeitenAnaphy EmanualLady MidnightNoch keine Bewertungen
- Tony - Electrolytes Lect NCMDokument84 SeitenTony - Electrolytes Lect NCMJoseph Nawen SindiongNoch keine Bewertungen
- Water MetabolismDokument3 SeitenWater MetabolismJuber mansuriNoch keine Bewertungen
- Revised Man As A Biological BeingDokument8 SeitenRevised Man As A Biological Beingapi-3832208Noch keine Bewertungen
- Medical Physiology: MMP 1215 (Part I)Dokument25 SeitenMedical Physiology: MMP 1215 (Part I)Kunda JosephNoch keine Bewertungen
- Water Chemistry: 1. Water Is A Polar MoleculeDokument2 SeitenWater Chemistry: 1. Water Is A Polar MoleculeRayn BougNoch keine Bewertungen
- Fluids Electrolytes Final Exam Topic 2Dokument231 SeitenFluids Electrolytes Final Exam Topic 2Kylle AlimosaNoch keine Bewertungen
- Water ReportingDokument29 SeitenWater ReportingShinrin SukehiroNoch keine Bewertungen
- Importance of WaterDokument11 SeitenImportance of WaterSasmitaNoch keine Bewertungen
- Water: The Most Precious Resource of Our Life: September 2015Dokument11 SeitenWater: The Most Precious Resource of Our Life: September 2015Justas JonusasNoch keine Bewertungen
- Bag - Isi Bu - Uut ElektrolitDokument13 SeitenBag - Isi Bu - Uut ElektrolitbianmanNoch keine Bewertungen
- Minister of Health Kafue College of Nursing and Midwifery Public Health NursingDokument9 SeitenMinister of Health Kafue College of Nursing and Midwifery Public Health NursingLawrence Favor SilungweNoch keine Bewertungen
- NCM 112 MW NotesDokument6 SeitenNCM 112 MW NotesJames Kristopher RebayaNoch keine Bewertungen
- Inorganic Compounds EssentialDokument12 SeitenInorganic Compounds EssentialGemeda GebinoNoch keine Bewertungen
- Cairan Dan ElektrolitDokument11 SeitenCairan Dan ElektrolitYuanitaipNoch keine Bewertungen
- Electrolytes PeriopDokument22 SeitenElectrolytes PeriopVivek PatangeNoch keine Bewertungen
- Lecture 1: Body Fluids & BloodDokument46 SeitenLecture 1: Body Fluids & BloodPriya BhattNoch keine Bewertungen
- MS Prelim ReviewerDokument5 SeitenMS Prelim Reviewerleslie_macasaetNoch keine Bewertungen
- Pathophysiology Module 4Dokument26 SeitenPathophysiology Module 4johnbryanmalonesNoch keine Bewertungen
- Fluid & ElectrolyteDokument18 SeitenFluid & Electrolytesaranya amuNoch keine Bewertungen
- Fe ConceptDokument177 SeitenFe ConceptIvan MaximusNoch keine Bewertungen
- Supercharging Autophagy - Based On The Teachings Of Dr. Eric Berg: Unleashing Its Full PotentialVon EverandSupercharging Autophagy - Based On The Teachings Of Dr. Eric Berg: Unleashing Its Full PotentialNoch keine Bewertungen
- Pure Water: The Science of Water, Waves, Water Pollution, Water Treatment, Water Therapy and Water EcologyVon EverandPure Water: The Science of Water, Waves, Water Pollution, Water Treatment, Water Therapy and Water EcologyNoch keine Bewertungen
- Defining The Concepts of Technology and Technology Transfer: A Literature Analysis Suzana Idayu Wati Osman Felda..Dokument12 SeitenDefining The Concepts of Technology and Technology Transfer: A Literature Analysis Suzana Idayu Wati Osman Felda..musawar420Noch keine Bewertungen
- Narrative Research: July 2020Dokument14 SeitenNarrative Research: July 2020musawar420Noch keine Bewertungen
- Pros and Cons of Sampling-With-Cover-Page-V2Dokument5 SeitenPros and Cons of Sampling-With-Cover-Page-V2musawar420Noch keine Bewertungen
- IJRRS Volume 2 Issue 1 Pages 23-34Dokument12 SeitenIJRRS Volume 2 Issue 1 Pages 23-34musawar420Noch keine Bewertungen
- Sampling - Methods With Cover Page v2Dokument4 SeitenSampling - Methods With Cover Page v2musawar420Noch keine Bewertungen
- Special Education Teacher Interview QuestionsDokument2 SeitenSpecial Education Teacher Interview Questionsmusawar420Noch keine Bewertungen
- Antennas Theory Design and Applications: Msee 4BDokument28 SeitenAntennas Theory Design and Applications: Msee 4Bmusawar420Noch keine Bewertungen
- A Resource Allocation Mechanism Based On WeightedDokument16 SeitenA Resource Allocation Mechanism Based On Weightedmusawar420Noch keine Bewertungen
- Health Effects Ofnon-Ionized Electromagnetic Radiation: Invited TalkDokument1 SeiteHealth Effects Ofnon-Ionized Electromagnetic Radiation: Invited Talkmusawar420Noch keine Bewertungen
- Can Teachers Discretion Enhance The Role of Professionalism in Times of Crisis A Comparative Policy Analysis of Distance Teaching in Italy andDokument12 SeitenCan Teachers Discretion Enhance The Role of Professionalism in Times of Crisis A Comparative Policy Analysis of Distance Teaching in Italy andmusawar420Noch keine Bewertungen
- This Review of The Article Has A Bearing On The Changes in Online Teaching As The COVIDDokument5 SeitenThis Review of The Article Has A Bearing On The Changes in Online Teaching As The COVIDmusawar420Noch keine Bewertungen
- Glaucoma and Short-Wavelength Light Sensitivity (Blue Light)Dokument12 SeitenGlaucoma and Short-Wavelength Light Sensitivity (Blue Light)musawar420Noch keine Bewertungen
- The Geopolitics of The Two Koreas and The United States Seen Through The North Korean Nuclear IssueDokument21 SeitenThe Geopolitics of The Two Koreas and The United States Seen Through The North Korean Nuclear Issuemusawar420Noch keine Bewertungen
- AkramHouraniThesisV3.1 201610518 PDFDokument295 SeitenAkramHouraniThesisV3.1 201610518 PDFmusawar420Noch keine Bewertungen
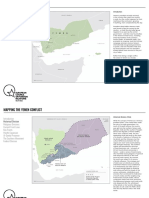
- Mapping YemenDokument9 SeitenMapping Yemenmusawar420Noch keine Bewertungen
- The Political Culture of DemocracyDokument32 SeitenThe Political Culture of Democracymusawar420Noch keine Bewertungen
- Rights of Minorities in Islam: From Dhimmis To CitizensDokument56 SeitenRights of Minorities in Islam: From Dhimmis To Citizensmusawar420Noch keine Bewertungen
- The Study of Democracy and DemocratizationDokument7 SeitenThe Study of Democracy and Democratizationmusawar420Noch keine Bewertungen
- Concept of Secularism: An Indian ScenarioDokument50 SeitenConcept of Secularism: An Indian Scenariomusawar420Noch keine Bewertungen
- Pak-US Relations A Historical Review, Munawar Hussain Footnotes CorrectedDokument16 SeitenPak-US Relations A Historical Review, Munawar Hussain Footnotes Correctedmusawar420Noch keine Bewertungen
- Literature Review On Venous Leg UlcersDokument8 SeitenLiterature Review On Venous Leg Ulcersafdtzwlzd100% (1)
- Research Proposal - Group 10Dokument14 SeitenResearch Proposal - Group 10Ngọc Diễm PhùngNoch keine Bewertungen
- Material Safety Data Sheet: Hayem's SolutionDokument7 SeitenMaterial Safety Data Sheet: Hayem's SolutionCherie DenielleNoch keine Bewertungen
- Miranda, Elizabeth S. - BSHM3B (GEC107 W4) .Dokument8 SeitenMiranda, Elizabeth S. - BSHM3B (GEC107 W4) .Grace Hermano ManiponNoch keine Bewertungen
- Teaching PE and Health Week 2Dokument51 SeitenTeaching PE and Health Week 2TEDLYN JOY ESPINONoch keine Bewertungen
- VE022 Personal Goal Achievement Yearly ReviewDokument3 SeitenVE022 Personal Goal Achievement Yearly ReviewLenard SusanoNoch keine Bewertungen
- Chootip 2017 Efficacy and Safety of "Yahom" As A Traditional Thai Herbal Therapy - A Systematic ReviewDokument14 SeitenChootip 2017 Efficacy and Safety of "Yahom" As A Traditional Thai Herbal Therapy - A Systematic ReviewAkarat SivaphongthongchaiNoch keine Bewertungen
- Oet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestDokument7 SeitenOet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestKrishna Ramas-MaddiNoch keine Bewertungen
- Standards For Lethality and StabilizationDokument18 SeitenStandards For Lethality and StabilizationtarunNoch keine Bewertungen
- Monitoring of Lgus On The Management of Covid-19 Related Health Care WastesDokument3 SeitenMonitoring of Lgus On The Management of Covid-19 Related Health Care WastesDann MarrNoch keine Bewertungen
- Research Paper On Youth SportsDokument10 SeitenResearch Paper On Youth Sportsapi-569130109Noch keine Bewertungen
- 219 503 1 SMDokument9 Seiten219 503 1 SMdwi antoNoch keine Bewertungen
- WA 2 - Case Study of Mandarin OrientalDokument7 SeitenWA 2 - Case Study of Mandarin OrientalOla leahNoch keine Bewertungen
- Kellogg Case StudyDokument4 SeitenKellogg Case StudyDrSachin SrivastavaNoch keine Bewertungen
- TIKTOKDokument10 SeitenTIKTOKLenny FebryanaNoch keine Bewertungen
- Registration Certificate Government of Tamil NaduDokument4 SeitenRegistration Certificate Government of Tamil NaduSanthosh DHAYANITHINoch keine Bewertungen
- Case Study No 3Dokument5 SeitenCase Study No 3ERICKA GRACE DA SILVANoch keine Bewertungen
- Whohgnwg85 10 PDFDokument34 SeitenWhohgnwg85 10 PDFbabyNoch keine Bewertungen
- Alfa ResultSubServices PDFDokument1 SeiteAlfa ResultSubServices PDFMenna AghanyNoch keine Bewertungen
- Pe Reviewer 2ND Sem MidtermDokument3 SeitenPe Reviewer 2ND Sem Midtermtaysonarlene.mhpnhsNoch keine Bewertungen
- Behavioral Marital ModelDokument16 SeitenBehavioral Marital ModelKrizzia Louise B. CabreraNoch keine Bewertungen
- Moral and Legal Status of AbortionDokument20 SeitenMoral and Legal Status of AbortionStarboiiNoch keine Bewertungen
- Kimberley Coastal Voyage: Darwin, AustraliaDokument2 SeitenKimberley Coastal Voyage: Darwin, AustraliaAustin Viel Lagman MedinaNoch keine Bewertungen
- (창사글) '인공지능 의료진단' 논문Dokument215 Seiten(창사글) '인공지능 의료진단' 논문yangjiwon041111Noch keine Bewertungen
- Latihan Soal Bahasa Inggris Sma HortatorDokument6 SeitenLatihan Soal Bahasa Inggris Sma HortatorErna TemkonNoch keine Bewertungen