Beruflich Dokumente
Kultur Dokumente
Children's Separation Anxiety Scale (CSAS) : Psychometric Properties
Hochgeladen von
Yeremias EdwinOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Children's Separation Anxiety Scale (CSAS) : Psychometric Properties
Hochgeladen von
Yeremias EdwinCopyright:
Verfügbare Formate
Children’s Separation Anxiety Scale (CSAS): Psychometric
Properties
Xavier Méndez1*, José P. Espada2, Mireia Orgilés2, Luis M. Llavona3, José M. Garcı́a-Fernández4
1 Department of Personality, Psychological Assessment and Treatment, University of Murcia, Murcia, Spain, 2 Department of Health Psychology, Miguel Hernández
University, Elche, Spain, 3 Department of Personality, Psychological Assessment and Treatment (Clinical Psychology), Complutense University, Madrid, Spain,
4 Department of Developmental Psychology and Teaching, University of Alicante, Alicante, Spain
Abstract
This study describes the psychometric properties of the Children’s Separation Anxiety Scale (CSAS), which assesses
separation anxiety symptoms in childhood. Participants in Study 1 were 1,908 schoolchildren aged between 8 and 11.
Exploratory factor analysis identified four factors: worry about separation, distress from separation, opposition to separation,
and calm at separation, which explained 46.91% of the variance. In Study 2, 6,016 children aged 8–11 participated. The
factor model in Study 1 was validated by confirmatory factor analysis. The internal consistency (a = 0.82) and temporal
stability (r = 0.83) of the instrument were good. The convergent and discriminant validity were evaluated by means of
correlations with other measures of separation anxiety, childhood anxiety, depression and anger. Sensitivity of the scale was
85% and its specificity, 95%. The results support the reliability and validity of the CSAS.
Citation: Méndez X, Espada JP, Orgilés M, Llavona LM, Garcı́a-Fernández JM (2014) Children’s Separation Anxiety Scale (CSAS): Psychometric Properties. PLoS
ONE 9(7): e103212. doi:10.1371/journal.pone.0103212
Editor: Ingmar H.A. Franken, Erasmus University Rotterdam, Netherlands
Received November 7, 2013; Accepted June 30, 2014; Published July 29, 2014
Copyright: ß 2014 Méndez et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This research was supported by the Spanish National Plan for Research, Development and Technological Innovation Grant (EDU2008-05060) awarded
to Xavier Méndez, and by BANCAJA-UMH Grant (2007-2009), awarded to Mireia Orgilés. The funders had no role in study design, data collection and analysis,
decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* Email: xmendezc@um.es
Introduction ment, self-report rating scales are widely used, together with
structured interviews, as they are easy to apply, fill out and
Separation anxiety disorder (SAD) in children is characterized evaluate. They are especially useful from the age of 7 onwards,
by excessive and inappropriate anxiety for the child’s stage of when the child has acquired sufficient reading ability and self-
development, and which he or she experiences on being separated assessment skills. There are general self-reports for assessing the
from attachment figures – generally the parents – or spending time different childhood anxiety disorders, including SAD, such as the
outside his or her home [1]. This disproportionate anxiety Screen for Child Anxiety Related Emotional Disorders (SCARED)
manifests itself in distress, worry and resistance to or rejection of [6] or the Spence Children’s Anxiety Scale (SCAS) [7]. The
the separation. Prevalence of SAD is 3.9% in childhood (6–12 comprehensive application of these instruments, which include
years) and 2.6% in adolescence (13–18 years), according to two more than 40 items, is of great use for screening in epidemiological
meta-analyses carried out with 13 and 26 epidemiological studies, studies, but may be unnecessary and excessive in clinical cases of
respectively [2]. SAD and some types of specific phobia, such as SAD, detected via interview; at the same time, application of just
those related to animals, are the anxiety disorders with earliest age the SAD scales, with their less than 10 items, may be insufficient
of onset, the majority of cases emerging prior to age 12 [3]. The for assessing the full spectrum of symptoms and drawing up a
presence of SAD in childhood predicts this same disorder in treatment plan. Therefore, the construction and validation of self-
adolescence (age 13–19) [4]. SAD is a strong risk factor (78.6%) for
reports for the specific assessment of SAD is relevant. There are
the development of psychopathology in young adulthood (age 19–
three self-reports of this type: the Separation Anxiety Assessment
30), so that the diagnosis, assessment and treatment of children
Scale (SAAS) [8], the Separation Anxiety Avoidance Inventory
with SAD are relevant for preventing the appearance of disorders
(SAAI) [9], and the Separation Anxiety Scale for Children (SASC)
such as panic and depression [5].
[10]. The SAAS has the disadvantage that its psychometric
Clinical diagnosis and assessment aspire to collect as much
properties have not yet been published, whilst the SAAI focuses
information as possible at the least possible cost in time and
exclusively on avoidant behaviors, neglecting subjective aspects,
money, and in effort for the child, parents and professionals.
such as distress and worry, both characteristic of SAD. Further-
Optimization of assessment efficiency involves the avoidance of
more, these two self-reports assess separation anxiety in both
extreme positions. On the one hand, excessively thorough
childhood and adolescence at the same time (6–17 and 4–15 years,
assessment leads to fatigue and to the risk of loss of precision
respectively), despite the fact that the symptoms vary with age.
and early abandonment of the therapeutic relation. On the other,
This is a problematic aspect, as it is inappropriate, for example, to
very brief assessment is of little use for planning treatment, and
present a four-year-old with item 2 of the SAAI, ‘‘Because I am
involves risks such as the omission of relevant data and premature
anxious, I avoid being at home alone in the evening’’, or a 17-
therapeutic decisions. In the framework of multi-method assess-
PLOS ONE | www.plosone.org 1 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
year-old with item 4 of the SAAS, ‘‘How often are you afraid to be head teachers and the school counselors, informing them verbally
left at home with a babysitter?’’ and in writing about the aim of the study, so as to obtain their
The SASC was developed for children aged 8 to 11 on the basis permission and encourage their cooperation. Finally, parents were
of the three-dimensional theory of anxiety [11], which, when informed by letter and requested to provide written consent for
applied to separation anxiety, postulates three inter-related their children to participate in the study. The written parental
components: a) cognitive, or worry that something bad will consent was provided for all minors participating.
happen to the child and/or to his/her parents, b) psychophysi- Participants. Random cluster sampling was carried out in
ological, or distress resulting from the feelings of distress generated two provinces in central and southern Spain, respectively. Primary
by excessive vegetative activation, and c) behavioral, or opposition units were provincial districts, secondary units were schools, and
to being separated from one’s parents and/or away from home. tertiary units were classrooms. We recruited 2,005 children from
The confirmatory factor analysis confirmed that the model of primary school grades 3 to 6 at 19 schools. A total of 97 (4.84%)
three correlated factors showed the best fit to the data, were excluded due to errors or omissions in their responses,
corroborating the factors Worry about separation and Distress because their parents failed to provide informed consent, or
from separation; however, contrary to what was expected, the because they were immigrants whose level of Spanish was too low.
third factor was not opposition, but rather Calm at separation. The sample was made up of 1,908 schoolchildren with a mean age
The child’s calm at separation from parents can be interpreted a) of 9.61 (SD = 1.11). The chi-squared test for homogeneity of the
cognitively, as the absence of worry – for example, I don’t think distribution of frequencies indicated that there were no statistically
my parents will have an accident or get sick; b) psychophysiolog- significant differences between the eight groups of gender x age in
ically, as the absence of distress – for example, I don’t have Table 1 (x2 = 0.48, df = 3, p = 0.92). Participants covered a wide
stomach-ache or feel like crying; c) behaviorally, as the absence of range of socio-economic status, which was determined according
opposition – for example, I don’t do things to check whether my to the school’s type (public, grant-assisted private or private) and
parents are OK or to try and be with them; d) positively, as the location (city, small town/village or village/rural).
presence of calmness – for example, I feel calm/OK when my Procedure. The researchers generated twenty new separa-
parents go away on a trip. The factor Calm at separation is tion anxiety items that were evaluated with the same procedure as
problematic not only from the theoretical point of view, but also in the original study [10]. A pilot study was carried out with a
methodologically, as the internal consistency coefficient (Cron- random sample of 103 children aged 8 to 11 (M = 9.37, SD = 1.06)
bach’s alpha) was low (0.63). Moreover, the SASC has other of both genders (54.43% girls). Six items were eliminated, a) at the
methodological limitations: explained variance was just 32.80%, suggestion of twelve experts in the psychopathology of develop-
concurrent validity was calculated solely with two self-reports – ment with broad clinical experience, and who acted as judges, b)
one of anxiety and another of fears at school –, and neither its because participants found them difficult to understand, and c) due
sensitivity nor its specificity was reported. to low item-test correlation. Examples of the eliminated items are
At a theoretical level it is interesting to explore whether ‘‘Do you refuse to sleep at a friend’s house?’’ and ‘‘Do you forget
opposition is a dimension of separation anxiety and whether calm your mom or dad when you go to an after-school activity?’’ The
is a positive factor that cannot be reduced to the mere absence of remaining 14 new items were added to the 26 original SASC items
worry, distress and/or opposition. It is also important to have to make up the bank of 40 items employed in this study.
access to a psychometrically satisfactory instrument that addresses Participants responded to the bank of 40 separation anxiety
the deficiencies of the SASC – specifically, one that improves the items in the classroom and within normal class time. The
construct validity by increasing the percentage of explained researchers’ assistants read the instructions aloud, provided
variance, that increases the convergent and discriminant validity individual help where necessary, and made sure that the pupils
on including measures of SAD, child anxiety, depression and answered their own questions independently. In order to avoid
anger, and that analyzes the structural validity by means of the bias, neither the assessors nor the participants were aware of the
sensitivity and specificity. Given the lack of a specific self-report study’s aims until the instruments had been handed in and
rating scale for childhood SAD with adequate psychometric processed.
properties, which assesses the varied symptomatology of this Measure. We administered the bank of 40 separation anxiety
disorder rather than focusing on just a single aspect of it, such as items, made up of the 26 original items of the SASC [10] plus the
avoidant behavior, the general objectives of this study, taking as a 14 new items of the pilot study, which evaluates childhood
starting point the SASC, were to develop (Study 1) and validate separation anxiety by means of a 5-point Likert scale, ranging
(Study 2) a self-report instrument, the Children’s Separation from 1 (never or almost never) to 5 (always or almost always).
Anxiety Scale (CSAS). In Study 1 we carry out an exploratory Data Analysis. The underlying structure of the CSAS was
factor analysis with a bank of 40 items: the 26 from the original identified by means of an iterative principal axis factor analysis
study [10] plus 14 new items from a pilot study. In Study 2 we with oblimin rotation because the factors were correlated. The
calculate the validity, reliability, sensitivity and specificity of the data analysis was carried out with the SPSS statistics package,
CSAS. version 20.0.
Study 1: Exploratory Factor Analysis Results
The criteria for obtaining the factorial solution were: a) to retain
Methods factors with eigenvalues higher than 1 (Kaiser criterion), b) to
Ethics Statement. The authors state that their research, assign to each factor the items that loaded higher than 0.40, and c)
approved by the Research Ethics Committee of the University of to include at least five items in each factor. Twenty items were
Murcia (Spain), has been performed in accordance with the ethical removed: nine because the saturation was under 0.40 (items 1, 3,
standards laid down in the 1964 Helsinki Declaration and its later 4, 6, 8, 13, 20, 22, and 32) and eleven because the corresponding
amendments. The education authorities were informed of the factor, which explained less than five per cent of the variance,
study goals, and authorization was requested. Once such included fewer than five items (items 7, 9, 10, 19, 30, 34, 35, 36,
authorization had been obtained, the researchers interviewed the 37, 38, and 40). Four factors, each with five items, were obtained,
PLOS ONE | www.plosone.org 2 July 2014 | Volume 9 | Issue 7 | e103212
Table 1. Exploratory factor analysis.
Item Factor 1 Factor 2 Factor 3 Factor 4 Factor 5 Factor 6 Factor 7 Factor 8
28. Do you worry about something bad happening to you? 0.77 20.04 0.11 20.01 0.07 20.01 0.01 0.06
21. Do you worry about something bad happening to your mom or dad? 0.76 0.01 0.03 0.05 0.04 0.10 0.11 0.02
25. Do you worry about your mom or dad having an accident? 0.74 20.11 0.07 20.01 0.05 20.01 0.01 0.10
39. Do you worry about having an accident? 0.70 0.07 20.02 0.00 20.04 20.03 20.05 20.13
PLOS ONE | www.plosone.org
31. Do you worry about getting sick? 0.67 0.10 0.03 0.14 0.15 0.13 0.17 20.02
20. Do you worry about getting lost? 0.35 0.01 0.28 0.25 0.15 0.24 0.18 0.01
13. Do you worry about your mom or dad getting sick? 0.31 0.12 0.18 20.13 20.02 20.08 20.13 20.04
26. Do you feel like crying when your mom or dad drops you off at school? 20.05 0.76 0.11 0.04 0.08 0.09 0.06 0.01
23. Do you feel bad when your mom or dad drops you off at school? 0.02 0.70 0.19 0.04 0.04 0.09 0.04 0.09
15. Do you feel bad at school because your mom or dad isn’t with you? 0.01 0.66 0.30 0.05 0.12 0.08 0.02 0.07
29. Are you afraid to eat at school in case you might vomit or choke? 0.08 0.62 0.01 0.06 0.16 0.03 0.26 0.05
16. Does your belly hurt when you have to leave your mom or dad? 20.05 0.57 0.30 0.03 0.24 0.13 0.00 20.10
32. Do you follow your mom or dad around the house? 0.03 0.34 0.19 0.02 0.09 0.34 0.04 0.06
12. Do you try to persuade your mom or dad not to go when he/she is planning to go on a trip? 0.08 0.20 0.66 0.07 0.02 0.03 0.24 0.05
18. Do you protest when your mom or dad plans to go out for the evening? 0.16 0.08 0.64 0.12 0.00 0.03 20.05 20.04
5. Do you protest when your mom or dad tells you he/she is going out? 0.12 0.08 0.60 0.05 0.15 20.01 0.29 0.12
3
2. Do you try to call to your mom or dad when he/she isn’t with you? 0.24 0.19 0.56 0.19 0.20 0.09 0.08 20.01
14. Do you get sad, cry and protest when you’re apart from your mom or dad? 20.04 0.16 0.52 20.01 0.08 0.13 0.10 0.06
6. Do you feel like crying when you’re not with your mom or dad? 0.03 0.37 0.39 0.10 0.12 0.18 20.01 20.01
3. Do you get a headache when you have to leave your mom or dad? 20.02 0.36 0.35 0.11 0.20 0.16 20.04 20.10
8. Do you worry that something bad will happen that stops you seeing your mom or dad again? 0.32 0.09 0.35 0.07 0.25 0.06 0.01 0.07
11. Are you calm when your mom or dad isn’t with you? 0.01 0.02 0.19 0.66 0.06 20.01 0.08 0.21
33. Are you calm when you’re a long way from home? 20.01 0.01 0.06 0.64 0.10 0.06 20.01 0.16
27. Are you calm when you go away on a trip without your mom or dad? 0.05 0.04 20.01 0.61 0.00 0.00 0.03 20.07
17. Are you calm even if you can’t call your mom or dad? 0.05 0.07 0.18 0.60 20.01 20.02 0.02 0.06
24. Are you calm when it gets dark and you’re not with your mom or dad? 20.01 0.04 20.13 0.59 20.01 0.04 20.04 20.06
1. Are you calm when your mom or dad goes away on a trip? 0.10 20.02 0.31 0.37 20.01 0.10 0.12 0.12
19. Do you have nightmares where something bad happens to your mom or dad? 0.08 0.22 0.15 0.06 0.75 0.06 0.07 0.08
7. Do you have nightmares where you’re taken away from your mom or dad by force? 0.04 0.19 0.25 0.02 0.70 0.08 0.02 0.01
34. Do you have nightmares where something bad happens to you? 0.20 0.14 0.06 0.00 0.69 0.14 0.11 0.07
38. Do you ask your mom or dad to leave the light on when you go to bed at night? 0.01 0.22 0.10 20.01 0.02 0.61 0.06 0.08
37. Are you frightened when you watch scary movies? 0.09 0.03 20.01 0.00 0.13 0.55 0.19 20.10
35. Are you afraid to stay at home alone? 0.13 0.21 0.29 0.07 0.10 0.49 0.16 0.02
4. Do you ask your mom or dad to sleep with you at night? 0.03 0.29 0.29 0.01 0.03 0.34 0.11 0.17
36. Do you refuse to go on camping trips? 20.02 0.12 0.05 0.06 0.05 0.18 0.67 20.04
Psychometric Properties of the CSAS
July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
explaining 46.91% of the variance. Factor 1, Worry about
Factor 8
separation (items 21, 25, 28, 31, and 39), explained 13.91% of
20.02
0.27
0.70
0.55
0.44
the variance. This is the cognitive component of anxiety, and
refers to worry that something bad might happen to the child and/
Factor 7
or to his/her parents. Factor 2, Distress from separation (items 15,
20.01
20.18
16, 23, 26, and 29), explains 12.32% of the variance. This is the
0.60
0.38
0.17
psychophysiological component, which includes uncomfortable
feelings, such as nausea or stomach ache, and the negative feelings
separation can generate, such as wanting to cry. Factor 3,
Factor 6 Opposition to separation (items 2, 5, 12, 14, and 18), explained
20.17
0.19
0.13
0.04
0.40
10.66% of the variance. This is the behavioral component, which
refers to reactions for avoiding separation from the parents. Factor
4, Calm at separation (items 11, 17, 24, 27, and 33), explained
Factor 5
10.02% of the variance, and is the positive component, which
reflects confidence in the child on being separated from his or her
0.03
0.05
0.10
0.03
0.11
parents and/or on being away from home. Table 1 shows the
CSAS factor structure.
Factor 4
Study 2: Confirmatory Factor Analysis, Reliability
20.05
20.05
0.08
0.19
0.18
and Validity
Methods
Factor 3
Participants. In a similar way to Study 1, a random cluster
20.03
sampling was carried out in two provinces of southeastern Spain.
0.04
0.18
0.09
0.27
A total of 6,302 schoolchildren were recruited, from primary
school grades 3 to 6, and 72 schools. In all, 286 (4.54%) were
excluded for reasons similar to those reported in the previous
Factor 2
study. Thus, the sample was made up of 6,016 children with a
20.05
0.36
0.10
0.09
0.10
mean age of 9.59 (SD = 1.12). The chi-squared test for homoge-
neity of the distribution of frequencies highlighted the absence of
statistically significant differences between the eight groups of
Factor 1
gender x age in Table 2 (x2 = 5.33, df = 3, p = 0.15). Socio-
20.04
20.11
economic status of the participants was similar to that of those in
0.11
0.03
0.17
Study 1.
Test-retest reliability was calculated with 1,926 children
randomly selected from the sample, who responded to the CSAS
again four weeks later. Diagnostic validity was calculated with 398
children also randomly selected from the sample, and who were
9. Do you think about going home to be with your mom or dad when you’re at school?
assessed individually by means of a semi-structured interview
based on the DSM-IV criteria.
22. Do you feel bad when your mom or dad leaves you at home with a babysitter?
Seventeen children were diagnosed with SAD through the
ADIS-IV-C interview, accounting for 4.27%. The numbers of
cases in the subsample used for this analysis (n = 398) were 8
children aged 8 (7.92%), 4 aged 9 (3.88%), 3 aged 10 (3.12%) and
10. Are you calm when you get up in the mornings to go to school?
2 aged 11 (2.04%). As regards the gender variable, 7 were boys
(3.55%) and 10 were girls (4.98%).
Procedure. The processes of informing the education
30. Are you calm when you sleep alone in your bedroom?
authorities, the head teachers and the parents, as well as those
of requesting authorization and informed consent and adminis-
tering the self-reports in the classroom, were similar to those
described in Study 1.
40. Do you refuse to sleep away from home?
With a view to avoiding too much disruption of the pupils’
normal curriculum, and also to minimizing errors caused by
doi:10.1371/journal.pone.0103212.t001
fatigue, administration time of the self-reports was restricted to one
hour. Thus, each participant responded, in the classroom
situation, to just three instruments: I) the CSAS; II) one of the
following, more extensive, self-reports (more than 30 items): the
SAAS [8], the SCARED [6], the SCAS [7], or the State–Trait
Table 1. Cont.
Anxiety Inventory for Children (STAIC) [12]; and III) one of the
following, briefer, self-reports (less than 30 items): the Childhood
Anxiety Sensitivity Index (CASI) [13], the School Fears Survey
Scale (SFSS) [14], the Children’s Depression Inventory (CDI) [15]
Item
or the State–Trait Anger Expression Inventory for Children and
Adolescents (STAXI-CA) [16]. Thus, all participants filled out the
PLOS ONE | www.plosone.org 4 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
Table 2. Child’s gender and age.
Age
8 (%) 9 (%) 10 (%) 11 (%) Total (%)
Study 1
Boys 212 (11.11) 233 (12.21) 250 (13.10) 275 (14.41) 970 (50.84)
Girls 200 (10.48) 222 (11.64) 255 (13.36) 261 (13.68) 938 (49.16)
Total 412 (21.59) 455 (23.85) 505 (26.47) 536 (28.09) 1,908 (100)
Study 2
Boys 672 (11.17) 757 (12.58) 751 (12.48) 905 (15.04) 3,085 (51.28)
Girls 676 (11.24) 705 (11.72) 757 (12.58) 793 (13.18) 2,931 (48.72)
Total 1,348 (22.41) 1,462 (24,30) 1,508 (25,07) 1,698 (28,22) 6,016 (100)
doi:10.1371/journal.pone.0103212.t002
CSAS, while each one of the eight self-reports was filled out by rating scales. It is composed of two 20-item subscales with three
approximately a quarter of them (see n for each self-report in response alternatives (1 = rarely, 2 = sometimes, 3 = often), which
Table 3). The self-reports and the order of administration were evaluate current level of anxiety (state) and chronic symptoms of
assigned at random to each classroom group (20–25 pupils). anxiety (trait). Internal consistency (Cronbach’s alpha) for the
Measures. With the aim of analyzing in detail the convergent present sample was 0.87 for both state anxiety and trait anxiety.
and discriminant validity of the CSAS, we used a wide range of CASI [13]. We applied the Spanish adaptation for children
self-reports to assess variables related to separation anxiety. aged 9 to 11 [21]. Sensitivity to anxiety is the fear of the anxiety
CSAS. We administered the scale of 20 items resulting from symptoms produced by the belief that the feelings of anxiety are
Study 1, which assesses the frequency of separation anxiety dangerous or harmful. It is considered to predispose the individual
symptoms on a 5-point scale: never or almost never (1), sometimes to the development of anxiety disorders. The instrument consists
(2), often (3), very often (4), always or almost always (5). of 18 items for assessing this risk factor with a 3-point Likert-type
SAAS [8]. We employed the Spanish translation made by the scale (1 = none, 2 = some, 3 = a lot), e.g. ‘‘It scares me when I feel
researchers, with the authors’ permission, using the back- like I am going to throw up’’. The internal consistency coefficient
translation method [17]. It consists of 34 items whose response for the sample in our study was 0.85.
options are: never (1), sometimes (2), most of the time (3), and all SFSS [14]. This was designed for children aged 8 to 11. The 25
the time (4). Total score on the scale is obtained by summing the items on school fears are assessed via a three-point scale: 0 (not at
four key symptom dimensions: fear of being alone, fear of all), 1 (a little), 2 (a lot). The scale includes fears related to SAD,
abandonment, somatic complaints/fear of physical illness, and such as ‘‘Separating from parents to go to school’’, and others
worry about calamitous events, plus the safety signals index and unrelated to the disorder, such as ‘‘Getting bad exam marks’’.
frequency of calamitous events (never, once, twice, three times or Persistent refusal to go to school because of fear of separation is
more). The subscales consist of 5 items, except for the safety signals one of the characteristics of SAD. Internal consistency of this
index, which consists of 9 items. Internal consistency of the scale instrument was good (a = 0.90).
for the present study (Cronbach’s alpha) was 0.88. CDI [15]. We used the Spanish adaptation for children and
SCARED [6]. We applied the Spanish translation for children adolescents aged 7 to 15 [22]. Depressed mood is often associated
aged 8 to 12 [18]. The original instrument contains 41 items with SAD. The CDI is the self-report most widely used for
grouped in five subscales that assess different childhood anxiety assessing depressive symptomatology in childhood. It consists of 27
disorders: somatic/panic (13 items), general anxiety (9 items), items with three response options, and the child must choose from
separation anxiety (8 items), social phobia (7 items), and school them the one that best describes him or her in the last two weeks.
phobia (4 items). Symptom frequency is assessed by means of a For the present sample the internal consistency was very high
three-point scale: 0 (almost never), 1 (sometimes), 2 (often). (Cronbach’s alpha = 0.95).
Internal consistency of the present sample was good (Cronbach’s STAXI-CA. Del Barrio and Aluja [16] adapted the STAXI-2
alpha = 0.90). [23] for children and adolescents aged 8 to 17. This instrument
SCAS [7]. We employed the Spanish adaptation for use with consists of 32 items in four 8-item subscales: state anger, trait
children aged 8 to 12 [19], which includes 38 items related to six anger, expression of anger, and control of anger. The child marks
childhood anxiety disorders: generalized anxiety disorder (6 items), the option that best describes him/her: 1 (a little), 2 (quite a lot), 3
panic attack/agoraphobia (9 items), social phobia (6 items), (a lot). In our study we used only the subscales state anger
separation anxiety disorder (6 items), obsessive-compulsive disor- (a = 0.93) and trait anger (a = 0.80). The relation with separation
der (6 items), and physical injury fears (5 items), plus 6 positive anxiety is expected to be lower than with state anxiety and with
items that act as ‘‘fillers’’, to offset the tendency to respond trait anxiety.
negatively. Frequency of each symptom is measured using a 4- Anxiety Disorders Interview Schedule for Children for DSM-IV
point scale: never (0), sometimes (1), often (2), always (3). Internal (ADIS-IV-C) [24], Spanish adaptation [25]. This is a semi-
consistency (Cronbach’s alpha) of the complete scale in the present structured interview, based on the diagnostic criteria of the DSM-
study was 0.88. IV, and which is widely used with children and adolescents aged 7
STAIC [12]. We applied the Spanish adaptation for children to 17. It contains modules on all anxiety disorders, including SAD
and adolescents aged 9 to 15 [20]. This instrument is one of the and school refusal, as well as dysthymia, major depressive disorder,
most well studied and commonly used general anxiety self-report attention-deficit/hyperactivity disorder, conduct disorder, and
PLOS ONE | www.plosone.org 5 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
Table 3. Correlation coefficients of the CSAS with other self-reports.
CSAS n = 6,016
1. Worry 2. Distress 3. Opposition 4. Calm Total
SAAS n = 1,540
Fear of being alone 0.13** 0.44** 0.39** 0.19** 0.46**
Fear of abandonment 0.18** 0.43** 0.39** 0.17** 0.52**
Somatic complaints/Fear of physical illness 0.20** 0.46** 0.36** 0.17** 0.56**
Worry about calamitous events 0.58** 0.24** 0.38** 0.22** 0.63**
Safety signals index 0.20** 0.52** 0.51** 0.24** 0.61**
Frequency of calamitous events 0.12** 0.18** 0.18** 0.10** 0.30**
Total 0.37** 0.54** 0.55** 0.27** 0.72**
SCARED n = 1,498
Somatic/Panic 0.21** 0.48** 0.47** 0.19** 0.55**
Generalized anxiety 0.28** 0.32** 0.35** 0.16** 0.38**
Separation anxiety 0.32** 0.54** 0.55** 0.37** 0.62**
Social phobia 0.21** 0.29** 0.34** 0.14** 0.50**
School phobia 0.10** 0.45** 0.29** 0.16** 0.28**
Total 0.32** 0.54** 0.55** 0.24** 0.64**
SCAS n = 1,511
Separation anxiety disorder 0.33** 0.41** 0.50** 0.38** 0.61**
Social phobia 0.23** 0.26** 0.28** 0.18** 0.41**
Obsessive/compulsive disorder 0.29** 0.32** 0.34** 0.20** 0.42**
Panic/Agoraphobia 0.18** 0.34** 0.34** 0.18** 0.38**
Physical injury fears 0.14** 0.22** 0.26** 0.16** 0.28**
Generalized anxiety disorder 0.32** 0.26** 0.32** 0.18** 0.44**
Total 0.34** 0.38** 0.44** 0.28** 0.55**
STAIC n = 1,467
State 20.01 0.27** 0.21** 0.22** 0.28**
Trait 0.19** 0.34** 0.37** 0.27** 0.42**
CASI n = 1,473 0.34** 0.41** 0.42** 0.23** 0.59**
SFSS n = 1,531 0.24** 0.26** 0.25** 0.16** 0.32**
CDI n = 1,527 0.11** 0.27** 0.22** 0.16** 0.27**
STAXI-CA n = 1,485
State 20.09** 0.07* 20.07* 0.09** 20.01
Trait 0.15** 0.17** 20.03 0.10** 0.15**
CSAS Children’s Separation Anxiety Scale, SAAS Separation Anxiety Assessment Scale, SCARED Screen for Child Anxiety Related Emotional Disorders, SCAS Spence
Children’s Anxiety Scale, STAIC State Trait Anxiety Inventory for Children, CASI Childhood Anxiety Sensitivity Index, SFSS School Fears Survey Schedule, CDI Children’s
Depression Inventory, STAXI State Trait Anger Expression Inventory.
*p#0.05 ** p#0.01.
doi:10.1371/journal.pone.0103212.t003
oppositional-defiant disorder. Each diagnosis is completed with a with the Pearson product-moment correlation coefficient. Sensi-
severity assessment made by the clinician using a nine-point scale, tivity and specificity were studied by means of a receiver operating
from 0 (none) to 8 (very severely disturbing/disabling). Twenty-five characteristic (ROC) curve and area under the curve (AUC). A
psychologists with Masters qualifications in child psychopathology 264 between-subjects analysis of variance was carried out for
and clinical psychology received intensive training in the use of the examining the differences by gender and age in separation anxiety.
ADIS-IV-C with the help of a specific manual [26]. In the present The analyses were carried out using the statistics packages SPSS
sample, the kappa coefficient obtained for SAD was 1 (perfect version 20.0, AMOS version 20.0 and MedCalc version 12.5.
agreement).
Data Analysis. The structure of the CSAS obtained in Study Results
1 was examined by means of confirmatory factor analysis. Internal Gender and Age Differences. In the total sample we found
consistency was calculated with Cronbach’s alpha coefficient, and a significant decrease in separation anxiety with age (F3,
a classical item analysis was carried out to obtain the correlations 6012 = 49.01, p,0.001). Mean score on the CSAS was 59.02
of the items with the corresponding factor and with the CSAS total (SD = 11.07) at age 8, 56.72 (SD = 12.34) at age 9, 54.63
score. Concurrent validity and test-retest reliability were calculated (SD = 11.77) at age 10 and 49.84 (SD = 11.73) at age 11.
PLOS ONE | www.plosone.org 6 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
Four correlated factors model; x2 Chi-Square test, df Degrees of freedom, p Probability, RMSEA Root Mean Square Error of Approximation, GFI Goodness of Fit Index, AGFI Adjusted Goodness of Fit Index, NFI Normed Fit Index, CFI
Magnitude of the differences was large between the children 8
aged and 11 (d = 0.80), moderate between those aged 9 and 11
(d = 0.57), and small in the remaining cases (d,0.50).
Girls’ mean score (M = 56.08, SD = 12.35) was significantly
0.46
0.80
0.92
TLI
—
higher than that of boys (M = 53.49, SD = 11.98), though the
difference was small (F1, 6014 = 12.37, p,0.001, d = 0.21). There
was no interaction between the gender and age variables (F3,
6012 = 0.47, p = 0.71).
Confirmatory Factor Analysis. Four alternative models
0.52
0.81
0.93
CFI
were assessed: 1) the null or independent model (M0); 2) the one-
—
factor model (M1), in which the 20 scale items were forced to load
in a general separation anxiety factor; 3) the uncorrelated four-
factor model (M4); and 4) the four correlated factors model (M4*).
To examine the adequacy of the assessed models we used six fit
0.52
0.80
0.93
NFI
indexes: the Root Mean Square Error of Approximation
—
(RMSEA), the Goodness of Fit Index (GFI), the Adjusted
Goodness of Fit Index (AGFI), the Normed Fit Index (NFI), the
Comparative Fit Index (CFI), and the Tucker-Lewis Index (TLI),
as well as the chi-square statistic (x2). Browne and Cudeck [27]
recommend a value of less than 0.05 for RMSEA. Hu and Bentler
AGFI
0.72
0.90
0.96
[28] suggest 0.95 for the NFI, CFI and TLI, as well as using a
—
combination of fit indexes in order to reduce both type I and II
errors. For GFI and AGFI, values above 0.90 are considered
acceptable (Table 4).
The chi-square statistic was significant, demonstrating a poor fit
for all the models. However, these values must be considered with
0.77
0.92
0.97
GFI
care, since the goodness of fit statistic x2 depends on the sample
size. This statistic is very powerful with large samples, and can
detect significant differences in spite of the fact that the models fit
the data well; therefore, we took into account other fit indexes.
The best fit of the models studied was shown by the four correlated
factors model, which gave acceptable values for RMSEA GFI,
AGFI, NFI, CFI and TLI. Table 5 shows the correlation
RMSEA
coefficients among factors and with the total score of the CSAS.
0.11
0.07
0.04
Internal Consistency and Item Analysis. The internal
—
consistency coefficients (Cronbach’s alpha) were 0.82 for the
CSAS, 0.83 for Factor 1, Worry about separation, 0.76 for Factor
2, Distress from separation, 0.72 for Factor 3, Opposition to
separation, and 0.75 for Factor 4, Calm at separation. The item-
0.00
0.00
0.00
0.00
subscale correlations were acceptable, with a range of 0.57 to 0.79.
p
All the items obtained an item-test correlation higher than 0.30,
indicating their adequate behavior. Table 6 shows the item-
subscale correlation (IS-R), the corrected item-subscale correlation
(IS-Rc), the item-test correlation (IT-R), the corrected item-test
Table 4. Fit indexes for confirmatory factor models.
correlation (IT-Rc), the mean (M), and the standard deviation (SD)
190
170
170
164
df
of the 20 CSAS items.
Test-retest Reliability. Test-retest reliability coefficients
were r = 0.83 for CSAS, r = 0.69 for Worry about separation,
r = 0.67 for Distress from separation, r = 0.70 for Opposition to
separation, and r = 0.66 for Calm at separation.
Comparative Fit Index, TLI Tucker-Lewis Index.
Convergent and Discriminant Validity. Table 3 shows the
correlation coefficients of the factors and the total CSAS score
with other self-reports. Correlation of the CSAS total score with
doi:10.1371/journal.pone.0103212.t004
16627.45
15617.79
3332.27
1347.58
other measures of separation anxiety, specifically with the SAAS
total score and with the score on the corresponding subscales of
x2
the SCARED and the SCAS were high, ranging between 0.61 and
0.72.
Analysis of the correlation coefficients of the CSAS and SAAS
also reveals a close relationship between the similar factors of the
two instruments, Worry about separation (CSAS) and Worry
about calamitous events (SAAS) (r = 0.58), Distress from separa-
Model
tion (CSAS) and Somatic complaints/Fear of physical illness
(SAAS) (r = 0.46), and Opposition to separation (CSAS) and Safety
M4*
M0
M1
M4
Signals Index (SAAS) (r = 0.51). Correlations of the Calm at
PLOS ONE | www.plosone.org 7 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
Table 5. Correlation matrix among factors and with CSAS total score.
1. Worry 2. Distress 3. Opposition 4. Calm Total
1. Worry ---- ---- ---- ---- ----
2. Distress 0.21* ---- ---- ---- ----
3. Opposition 0.27* 0.51* ---- ---- ----
4. Calm 0.12* 0.30* 0.37* ---- ----
Total 0.60* 0.65* 0.77* 0.70* ----
*p,0.001.
doi:10.1371/journal.pone.0103212.t005
separation (CSAS) factor, with no equivalent in the SAAS, were selecting the optimum cut-off point. For determining the positive
low with all the factors of the latter scale (r,0.25). predictive value (PPV) we calculated for each cut-off point the
Correlation of CSAS total score was good with anxiety percentage of children with SAD who actually met the diagnostic
sensitivity, higher with trait anxiety than with state anxiety, weak criteria for this disorder. For determining the negative predictive
with school fears and depression, very low with trait anger, and value (NPV) we calculated for each cut-off point the percentage of
non-existent with state anger. children without SAD who actually did not meet the diagnostic
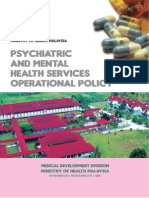
Sensitivity and Specificity. Sensitivity was operationalized criteria for this disorder. A receiver operating characteristic (ROC)
as the percentage of children with a SAD diagnosis according to curve and area under curve (AUC) were analyzed to establish the
the ADIS-IV-C who were correctly classified using the CSAS total optimal cut-off score. The results showed that the AUC for ROC
score. Specificity was operationalized as the percentage of children for the cut-off of 68 was 0.96 (95% CI, 0.93–0.98), and was
that did not receive a SAD diagnosis in the interview and were significant versus chance or a random ROC line (p,0.0001). This
correctly identified by the CSAS. The inverse relation between suggests that there is a 96% probability of a child with SAD
sensitivity and specificity requires equilibrium between the two for scoring higher on the CSAS than children without SAD.
Table 6. Item analysis of CSAS.
Items IS-R IS-RC IT-R IT-RC M SD
Factor 1: Worry about separation
21 0.79 0.60 0.45 0.34 4.33 1.19
28 0.75 0.63 0.45 0.36 4.01 1.43
31 0.75 0.49 0.33 0.24 4.24 1.27
25 0.73 0.58 0.38 0.28 4.42 1.17
39 0.68 0.54 0.46 0.44 3.69 1.55
Factor 2: Distress from separation
15 0.72 0.53 0.51 0.41 1.51 1.06
23 0.72 0.53 0.47 0.36 1.44 1.04
26 0.71 0.53 0.43 0.31 1.34 0.97
29 0.66 0.37 0.50 0.31 1.76 1.35
16 0.63 0.42 0.41 0.32 1.42 1.01
Factor 3: Opposition to separation
12 0.72 0.49 0.52 0.44 2.14 1.54
14 0.70 0.46 0.63 0.52 2.73 1.53
18 0.68 0.44 0.49 0.42 2.22 1.51
2 0.63 0.36 0.45 0.36 2.52 1.51
5 0.57 0.36 0.39 0.30 1.68 1.15
Factor 4: Calm at separation
11 0.69 0.42 0.43 0.35 2.92 1.60
17 0.64 0.39 0.37 0.33 3.09 1.60
33 0.63 0.38 0.35 0.28 2.88 1.60
27 0.62 0.35 0.31 0.24 3.21 1.61
24 0.58 0.37 0.31 0.23 3.18 1.64
IS-R Item-scale correlation, IS-Rc Corrected correlation item-scale, IT-R Item-test correlation, IT-Rc Corrected correlation item-test, M Mean, SD Standard deviation.
doi:10.1371/journal.pone.0103212.t006
PLOS ONE | www.plosone.org 8 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
specificity (95%, 95% CI, 92–97), a PPV of 76 and an NPV of
98. The Youden Index was 0.80 (Fig. 1).
Discussion
The CSAS comprises 20 items grouped in four factors: Worry
about separation, Distress from separation, Opposition to separa-
tion, and Calm at separation. In accordance with the three-
dimensional theory [11], the three first factors correspond to the
three response systems of anxiety, and permit assessment of the
symptomatology of SAD that is, excessive and persistent worry
about loss of or harm to attachment figures or the child him/
herself, excessive and recurrent distress in the child on being
separated from attachment figures, and resistance to or refusal to
accept separation from attachment figures. In contrast, Calm at
separation is a novel factor. Clinical psychologists expert in this
field, who judged the pertinence of the item bank in the original
study [10] with a view to controlling the tendency to respond
negatively, suggested the items of this subscale. It was expected
that on inverting the scores on the items they would distribute
themselves among the other factors according to whether the
anxiety was of a cognitive (worry), psychophysiological (distress) or
Figure 1. ROC curves of the CSAS. behavioral (opposition) nature. However, there emerged the Calm
doi:10.1371/journal.pone.0103212.g001 at separation factor, a positive dimension that reflects child’s self-
confidence in situations of separation. In some studies with
In order to assess the global diagnostic effectiveness we adolescent population [30,31] on Personal Report of Confidence
calculated the Youden Index [29], which is the maximum vertical as Speaker [32] it was found that confidence was not equivalent to
distance or the difference between the ROC curve and the a low level or absence of fear, but rather to self-confidence that
diagonal or chance line. The results revealed that a score of 68 in makes public-speaking a reinforcing activity (for example, ‘‘I face
the CSAS is the optimal cut-off, because it achieved the best the prospect of making a speech with complete confidence’’ or ‘‘At
balance, with good sensitivity (85%, 95% CI, 70–94) and the conclusion of a speech I feel that I have had a pleasant
Figure 2. Assessment and treatment of SAD.
doi:10.1371/journal.pone.0103212.g002
PLOS ONE | www.plosone.org 9 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
experience’’). Likewise, children differ not only in their level of the CSAS with the measures of anxiety, especially with those of
separation anxiety, but also in their degree of security and separation anxiety, is on the whole markedly greater than that with
enjoyment when they are home alone or they go away on a trip the CDI, reveals that the scale is an indicator of symptoms of
without their parents. The CSAS is the only self-report that anxiety, mainly of separation anxiety, more than depression. The
includes a positive dimension, and it would be interesting to study finding that the relation with trait anger is weak, and with state
the role of this dimension as a protection factor against SAD. anger is non-existent, also supports the discriminant validity of the
The Frequency of calamitous events of the SAAS shows the CSAS.
lowest correlations with the CSAS factors, since these events refer The present study has two important limitations. First, the
not to clinical characteristics, but to situations that trigger SAD. school sample recruited restricts generalization of the results, and
On the other hand, the Safety signals index, which is not second, the only source of information used was the child him/
considered a key symptom dimension, can be understood as herself. Future studies should analyze the psychometric properties
distress from or opposition to separation situations. The two SAAI of the CSAS with clinical samples and validate the version for
factors, Going to school, to bed alone (4 items) and Being or going parents, since SAD is a relational anxiety disorder – that is, it also
home alone when no-one is there (3 items) refer to the avoidance involves major attachment figures, so that multi-source assessment
of different separation situations. A study carried out with 931 of this childhood disorder is especially relevant.
parents of children aged 3 to 5 for evaluating early-onset In sum, the CSAS is a self-report that assesses the varied
separation anxiety found, together with a subjective fear and symptomatology of SAD, including the positive dimension Calm
worry factor, two factors of avoidance, one related to sleeping – for at separation, with good internal consistency, high temporal
example, ‘‘If your child wakes up during the night, does he/she stability, adequate convergent and discriminant validity, and good
call you insistently so that you have to go to his/her bedroom and sensitivity and specificity. It is an instrument that can be of great
calm him/her down? – and another related to everyday events – utility in the framework of multi-method assessment. Moreover, if
for example, ‘‘If you have to attend a meeting and leave your child it can be shown with clinical population that the psychometric
with a neighbor or friend for a few hours, does your child try to properties are similar, the CSAS would constitute a helpful tool in
resist?’’ [33,34]. Future research should explore whether the first- the context of diagnosis and treatment planning. Although the
order behavioral factor opposition/avoidance groups second-order focus of therapy for SAD is exposure, it is recommended that it be
factors defined by different separation situations: night, school, complemented with other therapeutic procedures so as to facilitate
home alone, etc. implementation, increase therapeutic collaboration and prevent
Internal consistency was good for the CSAS and for the Worry relapse. Coping Cat [41], a pioneering program in the treatment
about separation factor and adequate for the remaining factors. of childhood anxiety disorders, including SAD, facilitates exposure
Although the values are not high, they should be interpreted with various therapeutic strategies taught to children using the
taking into account that the factors are made up of just five items. acronym FEAR: Feeling frightened? (Relaxation), Expecting bad
These coefficients are similar to or higher than those found for things to happen? (Cognitive restructuring), Actions and attitudes
such short scales; thus, the internal consistency obtained with than can help (Problem-solving), Results and rewards (Self-
Cronbach’s alpha for the six-item factor Separation anxiety reinforcement). Similarly, the FRIENDS for Life program [42]
disorder of the SCAS was 0.70, 0.62 and 0.59 for school samples uses the acronym FRIENDS: Feeling worried? Relax and feel
from Australia [35], Belgium [36] and Spain, respectively [19]. good, Inner thoughts, Explore plans, Nice work, so reward
Temporal stability, with a test-retest interval of four weeks, was yourself, Don’t forget to practice, Stay calm, you know how to
also good for the CSAS and adequate for the factors. cope now. As regards parents, they are taught to reinforce
Correlation between the Worry about separation factor of the separation behaviors and extinguish their children’s complaints.
CSAS and the separation anxiety and generalized anxiety
Thus, the CSAS could guide selection of the coping skills and
subscales of the SCAS and SCARED are similar. This can be
family intervention to be applied – that is, cognitive restructuring if
explained, on the one hand, by the high level of comorbidity of
the SAD profile is worry, relaxation training if it is distress, and
childhood anxiety disorders [37] and, on the other, by the fact that
contingency management if it is opposition (see Fig. 2).
worry (e.g., about family members’ health) is an element common
to separation anxiety disorder and generalized anxiety disorder.
Correlation with the SFSS is not high. There is a long tradition Acknowledgments
that associates school refusal and SAD. In 1932, Broadwin [38] This research was supported by the Spanish National Plan for Research,
distinguished truancy from rejection to attend school out of fear Development and Technological Innovation Grant (EDU2008-05060)
that something will happen to one’s mother – or she might even awarded to Xavier Méndez, and by BANCAJA-UMH Grant (2007-2009),
die – if the child is not at home. However, only 22.2% of children awarded to Mireia Orgilés.
and adolescents with SAD refuse to go to school due to fear of
separation [39]. Schoolchildren are more afraid of failure and Author Contributions
punishment at school than of being separated from their parents to Conceived and designed the experiments: XM JPE MO LML JMG.
go to school [14]. Correlation with the CDI is explained by the Performed the experiments: XM JPE MO LML JMG. Analyzed the data:
substantial comorbidity of the SAD with childhood major XM JPE MO LML JMG. Contributed reagents/materials/analysis tools:
depressive disorder (37%) [40]. The fact that the correlation of XM JPE MO LML JMG. Wrote the paper: XM JPE MO LML JMG.
References
1. American Psychiatric Association (2013) Diagnostic and statistical manual of 3. Beesdo K, Knappe S, Pine DS (2009) Anxiety and anxiety disorders in children
mental disorders-IV, 5th ed. Washington, DC: Author. and adolescents: developmental issues and implications for DSM-V. Psychiatr
2. Costello EJ, Egger HL, Copeland W, Erkanli A, Angold A (2011) The Clin North Am 32: 483–524.
developmental epidemiology of anxiety disorders: phenomenology, prevalence, 4. Bittner A, Egger HL, Erkanli A, Costello EJ, Foley DL, et al. (2007) What do
and comorbidity. In: Silverman WK, Field AP, editors. Anxiety disorders in childhood anxiety disorders predict? J Child Psychol Psychiatry 48: 1174–1183.
children and adolescents, 2nd ed. New York: Cambridge University Press, pp.
56–75.
PLOS ONE | www.plosone.org 10 July 2014 | Volume 9 | Issue 7 | e103212
Psychometric Properties of the CSAS
5. Lewinsohn PM, Holm-Denoma JM, Small JW, Seeley JR, Joiner TE Jr (2008) 24. Silverman WK, Albano AM (1996) The Anxiety Disorders Interview Schedule
Separation anxiety disorder in childhood as a risk factor for future mental illness. for Children for DSM-IV: child and parent versions. San Antonio, TX:
J Am Acad Child Adolesc Psychiatry 47: 548–555. Psychological Corporation.
6. Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, et al. (1997) The Screen 25. Silverman WK, Albano AM, Sandı́n B (2001) Entrevista para el Diagnóstico de
for Child Anxiety Related Emotional Disorders (SCARED): scale construction los Trastornos de Ansiedad en Niños según el DSM-IV. ADIS-IV: C. Entrevista
and psychometric characteristics. J Am Acad Child Adolesc Psychiatry 36: 545– para el niño [The Anxiety Disorders Interview Schedule for Children for DSM-
553. IV. ADIS-IV: C. Child Interview]. Madrid: Klinik.
7. Spence SH (1997) Structure of anxiety symptoms among children: a 26. Sandı́n B (2002) Diagnóstico de los trastornos de ansiedad. Manual para la
confirmatory factor-analytic study. J Abnorm Psychol 106: 280–297. ADIS-IV: C/P [Diagnosis of anxiety disorders. Guidebook for ADIS-IV: C/P].
8. Eisen AR, Schaefer CE (2005) Separation anxiety in children and adolescents. Madrid: Klinik.
Guilford, New York 27. Browne MW, Cudeck R (1993) Alternative ways of assessing model fit. In: Bollen
9. In-Albon T, Meyer AH, Schneider S (2013) Separation Anxiety Avoidance KA, Long JS (eds) Testing structural equation models. Newbury Park, CA: Sage,
Inventory – child and parent version: psychometric properties and clinical utility pp. 136–162.
in a clinical and school sample. Child Psychiatry Hum Dev 44: 689–697. 28. Hu L, Bentler PM (1998) Fit indices in covariance structure modeling: sensitivity
10. Méndez X, Espada JP, Orgilés M, Hidalgo MD, Garcı́a-Fernández JM (2008). to underparameterized model misspecification. Psychol Methods 3: 424–453.
Psychometric properties and diagnostic ability of the separation anxiety scale for 29. Youden WJ (1950) Index for rating diagnostic tests. Cancer 3: 32–35.
children (SASC). Eur Child Adolesc Psychiatry 17: 365–372. 30. Méndez FX, Inglés CJ, Hidalgo MD (1999) Propiedades psicométricas del
11. Lang PJ (1968) Fear reduction and fear behavior: problems in treating a Cuestionario de Confianza para Hablar en Público: Estudio con una muestra de
construct. In: Shlien JM (ed) Research in psychotherapy. Washington, DC: alumnos de enseñanzas medias [Psychometric properties of the Personal Report
American Psychological Association, pp. 90–102. of Confidence as Speaker: A study with a sample of secondary education]
12. Spielberger CD (1973) Manual for the State–Trait Anxiety Inventory for Psicothema 11: 65–74.
Children. Palo Alto, CA: Consulting Psychologists Press. 31. Méndez FX, Inglés CJ, Hidalgo MD (2004) La version española abreviada del
13. Silverman WK, Fleisig W, Rabian B, Peterson RA (1991) Childhood Anxiety Cuestionario de Confianza para Hablar en Público: Fiabilidad y validez en
Sensitivity Index. J Clin Child Psychol 20: 162–168. población adolescente [The shortened Spanish version of the Personal Report of
14. Garcı́a-Fernández JM, Espada JP, Orgilés M, Méndez X (2010) Psychometric Confidence as Speaker: Reliability and validity in adolescent population] Behav
properties of the School Fears Survey Scale for preadolescents (SFSS-II). Psychol 12: 5–24.
Psicothema 22: 502–508.
32. Paul GL (1966) Insight vs desensitization in psychotherapy. Stanford, CA:
15. Kovacs M (1981) Rating scales to assess depression in school-aged children. Acta
Stanford University Press.
Paedopsychiatr 46: 305–315.
33. González MC (2003) Elaboración y validación del Cuestionario de Ansiedad por
16. Del Barrio V, Aluja A (2009) STAXI-NA: Inventario de Expresión de Ira
Separación de Inicio Temprano [Elaboration and validation of the Early Onset
Estado-Rasgo en Niños y Adolescentes [STAXI-CA: State–Trait Anger
Anxiety Separation Anxiety Questionnaire]. Dissertation, University of Murcia
Expression Inventory for Children and Adolescents]. Madrid: TEA.
17. Hambleton RK (2005) Issues, designs, and technical guidelines for adapting tests 34. Méndez X, Orgilés M, Espada JP (2008) Ansiedad por separación: psicopato-
into multiple languages and cultures. In: Hambleton RK, Merenda PF, logı́a, evaluación y tratamiento [Separation anxiety: psychopathology, assess-
Spielberger C (eds) Adapting educational and psychological tests for cross- ment and treatment]. Pirámide, Madrid
cultural assessment. London: Lawrence Erlbaum Associates, pp. 3–38. 35. Spence SH (1998) A measure of anxiety symptoms among children. Behav Res
18. Vigil-Colet A, Canals J, Cosı́ S, Lorenzo-Seva U, Ferrando PJ, et al. (2009) The Ther 36: 545–566.
factorial structure of the 41-item version of the Screen for Child Anxiety Related 36. Muris P, Merckelbach H, Ollendick TH, King NJ, Bogie N (2002) Three
Emotional Disorders (SCARED) in a Spanish population of 8 to 12 years-old. traditional and three new childhood anxiety questionnaires: their reliability and
Int J Clin Health Psychol 9: 313–327. validity in a normal adolescent sample. Behav Res Ther 40: 753–772.
19. Orgilés M, Méndez X, Spence SH, Huedo-Medina TB, Espada JP (2012) 37. Grills-Taquechel AE, Ollendick TH (2013) Phobic and anxiety disorders in
Spanish validation of the Spence Children’s Anxiety Scale. Child Psychiatry children and adolescents. Cambridge, MA: Hogrefe.
Hum Dev 43: 271–281. 38. Broadwin IT (1932) A contribution to the study of truancy. Am J Orthopsy-
20. Seisdedos N (2009) STAIC: Cuestionario de Autoevaluación Ansiedad Estado/ chiatry 2: 253–259.
Rasgo en Niños [STAIC: State–Trait Anxiety Inventory for Children], 4th ed. 39. Allen JL, Lavallee K, Herren C, Ruhe J, Schneider S (2010) DSM-IV criteria for
Madrid: TEA. childhood separation anxiety disorder: informant, age, and sex differences.
21. Sandı́n B, Chorot P, Santed MA, Valiente RM (2002) Análisis factorial J Anxiety Disor 24: 946–952.
confirmatorio del Índice de Sensibilidad a la Ansiedad para Niños [A 40. Shear K, Jin R, Ruscio AM, Walters EE, Kessler RC (2006) Prevalence and
confirmatory factor analysis of the Childhood Anxiety Sensitivity Index]. correlates of estimated DSM-IV child and adult separation anxiety disorder in
Psicothema 14: 333–339. the National Comorbidity Survey Replication (NCS-R). Am J Psychiatry 163:
22. Del Barrio V, Carrasco MA (2004) CDI: Inventario de Depresión Infantil [CDI: 1074–1083.
Children’s Depression Inventory]. Madrid: TEA. 41. Kendall PC (1990) Coping Cat workbook. Ardmore, PA: Workbook.
23. Spielberger CD (1999) Manual for the State–Trait Anger Expression Inventory, 42. Barrett PM (2004) Friends for Life: Group’s leader manual for children, 4th ed.,
STAXI-2. Odessa, FL: Psychological Assessment Resources. Brisbane: Australian Academic Press.
PLOS ONE | www.plosone.org 11 July 2014 | Volume 9 | Issue 7 | e103212
Das könnte Ihnen auch gefallen
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeVon EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNoch keine Bewertungen
- Bottesi Millon PdQ4Dokument17 SeitenBottesi Millon PdQ4Adina RaduNoch keine Bewertungen
- New Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)Von EverandNew Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)Noch keine Bewertungen
- Escala PhobiaDokument16 SeitenEscala PhobiaArshiyaNoch keine Bewertungen
- Q Never True Rarely True Sometimes True Often True Very Often True When I Was Growing UpDokument3 SeitenQ Never True Rarely True Sometimes True Often True Very Often True When I Was Growing UpAnn Lee'sNoch keine Bewertungen
- Junior EpqDokument22 SeitenJunior EpqsekiNoch keine Bewertungen
- CGAS Ratings GuideDokument9 SeitenCGAS Ratings Guidekevin stefano100% (1)
- BFQ-C - Psychometric Properties of The Big Five Questionnaire-ChildrenDokument115 SeitenBFQ-C - Psychometric Properties of The Big Five Questionnaire-ChildrenPantiru GianaNoch keine Bewertungen
- CGASDokument4 SeitenCGASDinny Atin AmanahNoch keine Bewertungen
- Vol.5 - Midnight DawnDokument28 SeitenVol.5 - Midnight DawnMa MelloNoch keine Bewertungen
- Personality Assessment ScreenerDokument11 SeitenPersonality Assessment ScreenerMay-Anne VillamorNoch keine Bewertungen
- Depression HandoutDokument1 SeiteDepression Handoutapi-290668891Noch keine Bewertungen
- Global Assessment of FunctioningDokument1 SeiteGlobal Assessment of FunctioningKen Carter100% (2)
- Wisc V InterpretationDokument8 SeitenWisc V InterpretationliekeschaferNoch keine Bewertungen
- The Childhood Trauma Questionnaire in ADokument15 SeitenThe Childhood Trauma Questionnaire in ATuấn KhangNoch keine Bewertungen
- Anxiety DisorderDokument33 SeitenAnxiety DisorderMahmoud SalehNoch keine Bewertungen
- ResumenDokument1 SeiteResumensaraNoch keine Bewertungen
- CBT Adolescents Participants Manual EngDokument74 SeitenCBT Adolescents Participants Manual EngCarlos MoralesNoch keine Bewertungen
- The Adult Autism Spectrum Quotient (AQ) Ages 16+: Specimen, For Research Use OnlyDokument4 SeitenThe Adult Autism Spectrum Quotient (AQ) Ages 16+: Specimen, For Research Use Onlydanielaica21Noch keine Bewertungen
- DD CGAS For Children With PDDs - 03!02!2007Dokument5 SeitenDD CGAS For Children With PDDs - 03!02!2007Ryan GapNoch keine Bewertungen
- Selected Level 1 and 2 ASD Screening Measures: A B C B CDokument2 SeitenSelected Level 1 and 2 ASD Screening Measures: A B C B CJennie McCoolNoch keine Bewertungen
- Obsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsDokument6 SeitenObsessive Compulsive Inventory-Child Version (OCI-CV) in A Spanish Community Sample of Children and AdolescentsJorge VelardeNoch keine Bewertungen
- Ysrprofile PDFDokument5 SeitenYsrprofile PDFSonia Esteves100% (1)
- Scas Preschool Scale PDFDokument2 SeitenScas Preschool Scale PDFmuhammad al ihsanNoch keine Bewertungen
- Pai Adolescent Sample1Dokument9 SeitenPai Adolescent Sample1diablero999Noch keine Bewertungen
- Iq and AdaptativeDokument27 SeitenIq and AdaptativeRaul Morales VillegasNoch keine Bewertungen
- CAARS Patient EnglishDokument2 SeitenCAARS Patient Englishramav99759Noch keine Bewertungen
- Communication QuestionnaireDokument2 SeitenCommunication QuestionnaireKateřina ZábojníkováNoch keine Bewertungen
- AQ ChildDokument3 SeitenAQ ChildClaudia González MirandaNoch keine Bewertungen
- Shaywitz Et Al 2008 The Education of Dislexic Children PDFDokument30 SeitenShaywitz Et Al 2008 The Education of Dislexic Children PDFCatyta123Noch keine Bewertungen
- NCBRF ScoreSheetDokument3 SeitenNCBRF ScoreSheetPryscilla Ugas WisnarNoch keine Bewertungen
- SCASDokument3 SeitenSCASJyothi KNoch keine Bewertungen
- ADHD in The Classroom: Effective Intervention StrategiesDokument9 SeitenADHD in The Classroom: Effective Intervention Strategiesblanca_dhNoch keine Bewertungen
- Briere ITCT-A Final PDFDokument119 SeitenBriere ITCT-A Final PDFDave HenehanNoch keine Bewertungen
- Young's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsDokument35 SeitenYoung's Schema Questionnaire - Short Form Version 3 (YSQ-S3) : Preliminary Validation in Older AdultsFiona DayNoch keine Bewertungen
- Mathers Clinic Dysfunctional Attitude ScaleDokument6 SeitenMathers Clinic Dysfunctional Attitude ScaleGraça Maria Ferreira CarvalhoNoch keine Bewertungen
- The Autism Observation Scale For Infants: Scale Development and Reliability DataDokument8 SeitenThe Autism Observation Scale For Infants: Scale Development and Reliability DataRenata de Mesquita Ferraz LucenaNoch keine Bewertungen
- Trs-A: Teacher Rating Scales-Adolescent AgesDokument2 SeitenTrs-A: Teacher Rating Scales-Adolescent AgesEspíritu Ciudadano100% (1)
- Parent-Guardian-Rated DSM-5 Level 1 Cross-Cutting SymptomDokument1 SeiteParent-Guardian-Rated DSM-5 Level 1 Cross-Cutting SymptomGBNoch keine Bewertungen
- Pbeck Anxiety Inventory - Anxiety TestDokument3 SeitenPbeck Anxiety Inventory - Anxiety TestMilos Matic0% (1)
- CTQ EnglishDokument1 SeiteCTQ Englishmayra almaNoch keine Bewertungen
- WISC-III and Wppsi-R Assessment: Alan Kaufman Elizabeth O. LichtenbergerDokument8 SeitenWISC-III and Wppsi-R Assessment: Alan Kaufman Elizabeth O. LichtenbergermarisaNoch keine Bewertungen
- Dass 21Dokument2 SeitenDass 21Djennifer JacomelliNoch keine Bewertungen
- Kindergarten 1st Grade 2nd Grade: Chinook Open Optional Supply List 2022-23 School YearDokument2 SeitenKindergarten 1st Grade 2nd Grade: Chinook Open Optional Supply List 2022-23 School Yearapi-254776578Noch keine Bewertungen
- Marital Satisfaction Inventory, Revised (MSI-R)Dokument5 SeitenMarital Satisfaction Inventory, Revised (MSI-R)unicorn1979Noch keine Bewertungen
- Información Sobre El Test CDIDokument3 SeitenInformación Sobre El Test CDIMariellaNoch keine Bewertungen
- Benton VRT PDFDokument134 SeitenBenton VRT PDFabc123-1100% (1)
- Snap IV Instructions PDFDokument2 SeitenSnap IV Instructions PDFCamila Andrea Bravo BugueñoNoch keine Bewertungen
- PANSSDokument2 SeitenPANSSShawn MooneyNoch keine Bewertungen
- CAARS Observer EnglishDokument2 SeitenCAARS Observer Englishramav99759Noch keine Bewertungen
- WISC-V UK Interpretive Report - 24511549 - 20230215125433537Dokument19 SeitenWISC-V UK Interpretive Report - 24511549 - 20230215125433537Maha Abdul Kader100% (1)
- ADHD Diagnosis in AdultsDokument6 SeitenADHD Diagnosis in AdultsBrahim MehadjiNoch keine Bewertungen
- Screening MMSE PaediatricsDokument14 SeitenScreening MMSE PaediatricsFrancisco J. RapelaNoch keine Bewertungen
- Diagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Dokument17 SeitenDiagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Betania MendozaNoch keine Bewertungen
- Let's Play Minecraft!: Brought To You byDokument15 SeitenLet's Play Minecraft!: Brought To You byLaura DumitrescuNoch keine Bewertungen
- About TheDokument9 SeitenAbout TheGabby CrystalNoch keine Bewertungen
- Sample: M-Paci Millon Pre-Adolescent Clinical Inventory Interpretive ReportDokument7 SeitenSample: M-Paci Millon Pre-Adolescent Clinical Inventory Interpretive ReportNana LoVeNoch keine Bewertungen
- LPOW Thermometer ManualDokument12 SeitenLPOW Thermometer ManualShark LaserNoch keine Bewertungen
- RIAS™ Score Report: RIAS Subtest Scores/Index SummaryDokument6 SeitenRIAS™ Score Report: RIAS Subtest Scores/Index Summaryzaid zainudinNoch keine Bewertungen
- 16PF BibDokument10 Seiten16PF BibdocagunsNoch keine Bewertungen
- Commuting and Communication: An Investigation of Taxi Drivers' Experiences, Attitudes and Beliefs About Passengers With Communication DisordersDokument8 SeitenCommuting and Communication: An Investigation of Taxi Drivers' Experiences, Attitudes and Beliefs About Passengers With Communication DisordersYeremias EdwinNoch keine Bewertungen
- Interactions Between Physicians and Industry:: A Guide For CliniciansDokument9 SeitenInteractions Between Physicians and Industry:: A Guide For CliniciansYeremias EdwinNoch keine Bewertungen
- Malingering or Simulation in Ophthalmology - Visual AcuityDokument9 SeitenMalingering or Simulation in Ophthalmology - Visual AcuityYeremias EdwinNoch keine Bewertungen
- Ni Hms 290021Dokument17 SeitenNi Hms 290021AleCsss123Noch keine Bewertungen
- HHS Public AccessDokument21 SeitenHHS Public AccessYeremias EdwinNoch keine Bewertungen
- Access To Means of Suicide, Occupation and The Risk of Suicide: A National Study Over 12 Years of Coronial DataDokument7 SeitenAccess To Means of Suicide, Occupation and The Risk of Suicide: A National Study Over 12 Years of Coronial DataYeremias EdwinNoch keine Bewertungen
- Occupation and Mental Health in A National UK SurveyDokument10 SeitenOccupation and Mental Health in A National UK SurveyYeremias EdwinNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument14 SeitenNIH Public Access: Author Manuscriptyeremias setyawanNoch keine Bewertungen
- 5 PDFDokument8 Seiten5 PDFYeremias EdwinNoch keine Bewertungen
- Research ArticleDokument6 SeitenResearch Articleyeremias setyawanNoch keine Bewertungen
- 2 PDFDokument8 Seiten2 PDFYeremias EdwinNoch keine Bewertungen
- HHS Public AccessDokument20 SeitenHHS Public AccessYeremias EdwinNoch keine Bewertungen
- NIH Public Access: The Relationship Between Separation Anxiety and ImpairmentDokument12 SeitenNIH Public Access: The Relationship Between Separation Anxiety and Impairmentyeremias setyawanNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument19 SeitenNIH Public Access: Author ManuscriptYeremias EdwinNoch keine Bewertungen
- Gender Differences in Violence and Aggression - A Neurobiological PerspectiveDokument5 SeitenGender Differences in Violence and Aggression - A Neurobiological PerspectiveAndreeaTrandafirNoch keine Bewertungen
- Postpartum Depression: How Childbirth Educators Can Help Break The SilenceDokument9 SeitenPostpartum Depression: How Childbirth Educators Can Help Break The SilenceLecery Sophia WongNoch keine Bewertungen
- Aggression in Adolescence: A Gender PerspectiveDokument19 SeitenAggression in Adolescence: A Gender PerspectiveYeremias EdwinNoch keine Bewertungen
- The Prevalence and Correlates of Adult Separation Anxiety Disorder in An Anxiety ClinicDokument7 SeitenThe Prevalence and Correlates of Adult Separation Anxiety Disorder in An Anxiety ClinicMaysoun AtoumNoch keine Bewertungen
- 5 Gender Differences in Violence and AggressionDokument14 Seiten5 Gender Differences in Violence and AggressionYeremias EdwinNoch keine Bewertungen
- Violence Journal of Interpersonal: School Students Gender and Age Differences in Self-Reported Aggression of HighDokument18 SeitenViolence Journal of Interpersonal: School Students Gender and Age Differences in Self-Reported Aggression of HighYeremias EdwinNoch keine Bewertungen
- Treatment of Schizophrenia: Past, Present and Future: Bulletin of Clinical Psychopharmacology July 2015Dokument6 SeitenTreatment of Schizophrenia: Past, Present and Future: Bulletin of Clinical Psychopharmacology July 2015Yeremias EdwinNoch keine Bewertungen
- Depression in Pregnant Women and Mothers: How Children Are AffectedDokument3 SeitenDepression in Pregnant Women and Mothers: How Children Are AffectedYeremias EdwinNoch keine Bewertungen
- Abuse Port GuideDokument28 SeitenAbuse Port GuideBill DeWeeseNoch keine Bewertungen
- Integrated Treatment of Schizophrenia: Il Trattamento Integrato Della SchizofreniaDokument26 SeitenIntegrated Treatment of Schizophrenia: Il Trattamento Integrato Della SchizofreniaArya DibyoNoch keine Bewertungen
- BMC PsychiatryDokument5 SeitenBMC Psychiatryyeremias setyawanNoch keine Bewertungen
- Artigo EsquizofreniaDokument8 SeitenArtigo EsquizofreniaTaisa Fernanda LossNoch keine Bewertungen
- From Stack-Firing To Pyromania: Medico-Legal Concepts of Insane Arson in British, US and European Contexts, c.1800-1913. Part 2Dokument21 SeitenFrom Stack-Firing To Pyromania: Medico-Legal Concepts of Insane Arson in British, US and European Contexts, c.1800-1913. Part 2yeremias setyawanNoch keine Bewertungen
- Depresi Post PartumDokument4 SeitenDepresi Post PartumMeidy RamschieNoch keine Bewertungen
- Behaviour Research and TherapyDokument10 SeitenBehaviour Research and TherapyYeremias EdwinNoch keine Bewertungen
- EmotionaryDokument1 SeiteEmotionaryMarceCoelloNoch keine Bewertungen
- Beblo, Sinnamon & Baune - Specifying The Neuropsychology of Affective Disorders - Neuropsychology Reviews - 2011Dokument23 SeitenBeblo, Sinnamon & Baune - Specifying The Neuropsychology of Affective Disorders - Neuropsychology Reviews - 2011Roberta Finamore de AraujoNoch keine Bewertungen
- Zeeshan and AslamDokument11 SeitenZeeshan and AslamDian Atnantomi WiliyantoNoch keine Bewertungen
- Behaviour and Classroom Management Exam QuestionsDokument6 SeitenBehaviour and Classroom Management Exam QuestionsHoward Yoong90% (10)
- Schizophrenia BrochureDokument3 SeitenSchizophrenia BrochureFarhana SobriNoch keine Bewertungen
- Unit 1 AP PsychologyDokument6 SeitenUnit 1 AP PsychologyChristopher BradleyNoch keine Bewertungen
- A Review of The Literature On Evidence-Based Practice in PhysicalDokument10 SeitenA Review of The Literature On Evidence-Based Practice in PhysicalDyah SafitriNoch keine Bewertungen
- School NeuropsychologyDokument13 SeitenSchool NeuropsychologyAstrith Hernandez Mendoza100% (1)
- HW 2Dokument16 SeitenHW 2api-371944008Noch keine Bewertungen
- Counseling ImpDokument135 SeitenCounseling ImpAnanta ChaliseNoch keine Bewertungen
- Sensory Rooms Autism Reference ListDokument3 SeitenSensory Rooms Autism Reference ListMiss MarijaNoch keine Bewertungen
- Benefits of Physical Activity For Mental HealthDokument2 SeitenBenefits of Physical Activity For Mental HealthAna Sofia Sastoque PeñaNoch keine Bewertungen
- Social Anxiety DisorderDokument3 SeitenSocial Anxiety Disorderapi-269450159Noch keine Bewertungen
- IGNOU Psychology BA PracticalDokument27 SeitenIGNOU Psychology BA Practicalashish198150% (6)
- Developmentally Appropriate Child GuidanceDokument6 SeitenDevelopmentally Appropriate Child Guidanceapi-236047854Noch keine Bewertungen
- Topic Basic Concepts in PsychologyDokument18 SeitenTopic Basic Concepts in Psychologyloliman77100% (3)
- PDR As 1ed Index PrefaceDokument4 SeitenPDR As 1ed Index PrefaceSatish PrabhuNoch keine Bewertungen
- Preschool Assessment For AutismDokument14 SeitenPreschool Assessment For AutismFrancivaldo LourençoNoch keine Bewertungen
- Combined Behavioral Intervention (CBI) : Project COMBINEDokument360 SeitenCombined Behavioral Intervention (CBI) : Project COMBINEКонстантин КрахмалевNoch keine Bewertungen
- Social Psychology Kassin 9th Edition Test BankDokument26 SeitenSocial Psychology Kassin 9th Edition Test Bankyeseul jung100% (2)
- Bloom The Grief That Dare Not Speak Its NameDokument22 SeitenBloom The Grief That Dare Not Speak Its Nameciobanusimona25997075% (4)
- Module-2 Diass QTR1Dokument12 SeitenModule-2 Diass QTR1Trisha VenturaNoch keine Bewertungen
- Novel Tools and Resources For Evidence-Based Practice in PsychologyDokument10 SeitenNovel Tools and Resources For Evidence-Based Practice in PsychologyAndrea Despistes HerreraNoch keine Bewertungen
- Top 10 Stress Management Techniques For StudentsDokument27 SeitenTop 10 Stress Management Techniques For StudentsGeorgia GiampNoch keine Bewertungen
- Case Report of BGTDokument5 SeitenCase Report of BGTZainub A KhanNoch keine Bewertungen
- AsmrDokument4 SeitenAsmrafasfasdfNoch keine Bewertungen
- Theories of CounsellingDokument15 SeitenTheories of CounsellingMugambi Oliver100% (1)
- Counseling ReportDokument15 SeitenCounseling ReportMinagaFathmaSonnaya100% (1)
- Psychiatry Operational PolicyDokument124 SeitenPsychiatry Operational PolicyFarah Nasyitah100% (2)
- 2018 - Beeber - A Brief History of Davanloo's IstdpDokument10 Seiten2018 - Beeber - A Brief History of Davanloo's IstdpJohnNoch keine Bewertungen
- The Stoic Mindset: Living the Ten Principles of StoicismVon EverandThe Stoic Mindset: Living the Ten Principles of StoicismBewertung: 4.5 von 5 Sternen4.5/5 (10)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (28)
- The 7 Habits of Highly Effective People: The Infographics EditionVon EverandThe 7 Habits of Highly Effective People: The Infographics EditionBewertung: 4 von 5 Sternen4/5 (2475)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- Maktub: An Inspirational Companion to The AlchemistVon EverandMaktub: An Inspirational Companion to The AlchemistBewertung: 4.5 von 5 Sternen4.5/5 (3)
- The Mountain is You: Transforming Self-Sabotage Into Self-MasteryVon EverandThe Mountain is You: Transforming Self-Sabotage Into Self-MasteryBewertung: 4.5 von 5 Sternen4.5/5 (882)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesVon EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesBewertung: 5 von 5 Sternen5/5 (1635)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)
- Summary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearVon EverandSummary of Atomic Habits: An Easy and Proven Way to Build Good Habits and Break Bad Ones by James ClearBewertung: 4.5 von 5 Sternen4.5/5 (560)
- The Power of Now: A Guide to Spiritual EnlightenmentVon EverandThe Power of Now: A Guide to Spiritual EnlightenmentBewertung: 4.5 von 5 Sternen4.5/5 (4125)
- Breaking the Habit of Being YourselfVon EverandBreaking the Habit of Being YourselfBewertung: 4.5 von 5 Sternen4.5/5 (1459)
- Summary of The 48 Laws of Power: by Robert GreeneVon EverandSummary of The 48 Laws of Power: by Robert GreeneBewertung: 4.5 von 5 Sternen4.5/5 (233)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelVon EverandNo Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems ModelBewertung: 5 von 5 Sternen5/5 (4)
- Seven Spiritual Laws of Success: A Practical Guide to the Fulfillment of Your DreamsVon EverandSeven Spiritual Laws of Success: A Practical Guide to the Fulfillment of Your DreamsBewertung: 4.5 von 5 Sternen4.5/5 (1549)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessVon EverandThe Compound Effect by Darren Hardy - Book Summary: Jumpstart Your Income, Your Life, Your SuccessBewertung: 5 von 5 Sternen5/5 (456)
- The Freedom of Self-Forgetfulness: The Path to True Christian JoyVon EverandThe Freedom of Self-Forgetfulness: The Path to True Christian JoyBewertung: 5 von 5 Sternen5/5 (193)
- Becoming Supernatural: How Common People Are Doing The UncommonVon EverandBecoming Supernatural: How Common People Are Doing The UncommonBewertung: 5 von 5 Sternen5/5 (1480)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Summary of Cal Newport's Slow ProductivityVon EverandSummary of Cal Newport's Slow ProductivityBewertung: 4 von 5 Sternen4/5 (1)