Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Corin, From Symbols To ExperienceDokument48 SeitenCorin, From Symbols To Experiencerachel.avivNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- ELLIOTT - Pursued by Happiness and Beaten Senseless Prozac and The American DreamDokument6 SeitenELLIOTT - Pursued by Happiness and Beaten Senseless Prozac and The American Dreamrachel.avivNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Fromm Reichmann, LonelinessDokument16 SeitenFromm Reichmann, Lonelinessrachel.avivNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Bray, The Anorexic BodyDokument18 SeitenBray, The Anorexic Bodyrachel.avivNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- 05 Moncrieff Rethinking PsychotropicDokument11 Seiten05 Moncrieff Rethinking Psychotropicrachel.avivNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Cohen, Discontinuing DrugsDokument10 SeitenCohen, Discontinuing Drugsrachel.avivNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Bossewitch Columbia DisserationDokument324 SeitenBossewitch Columbia Disserationrachel.avivNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Conrad, The Discovery of HyperkinesisDokument11 SeitenConrad, The Discovery of Hyperkinesisrachel.avivNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Which Way Madness LiesDokument9 SeitenWhich Way Madness Liesrachel.avivNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Kemens, Postcolonialism and AntipsychDokument14 SeitenKemens, Postcolonialism and Antipsychrachel.avivNoch keine Bewertungen
- Hacking, Making Up PeopleDokument8 SeitenHacking, Making Up Peoplerachel.avivNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Arafae, Efficacy of SertralineDokument6 SeitenArafae, Efficacy of Sertralinerachel.avivNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Hyman, Diagnosis of Mental DisordersDokument27 SeitenHyman, Diagnosis of Mental Disordersrachel.avivNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Loenstein, Dissociative AmnesiaDokument31 SeitenLoenstein, Dissociative Amnesiarachel.avivNoch keine Bewertungen
- Hoch, Content of Depressive Ideas in Indian Patients PDFDokument9 SeitenHoch, Content of Depressive Ideas in Indian Patients PDFrachel.avivNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hartnack, Freud On Garuda's Wings PDFDokument1 SeiteHartnack, Freud On Garuda's Wings PDFrachel.avivNoch keine Bewertungen
- Jain, A Disgrace PDFDokument21 SeitenJain, A Disgrace PDFrachel.avivNoch keine Bewertungen
- The Impact of Psychopharmacology On Contemporary Psychiatry by Ross J BaldessariniDokument6 SeitenThe Impact of Psychopharmacology On Contemporary Psychiatry by Ross J Baldessarinirachel.avivNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Kakar, Reflections - On - Psychoanalysis, PDFDokument9 SeitenKakar, Reflections - On - Psychoanalysis, PDFrachel.avivNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Jain, Psychological Symptoms PDFDokument11 SeitenJain, Psychological Symptoms PDFrachel.avivNoch keine Bewertungen
- Greyson, NDE and SpiritualityDokument23 SeitenGreyson, NDE and Spiritualityrachel.avivNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hancock, Saintly Careers PDFDokument17 SeitenHancock, Saintly Careers PDFrachel.avivNoch keine Bewertungen
- Dahl, Reconstructing and Deconstructing The Self PDFDokument9 SeitenDahl, Reconstructing and Deconstructing The Self PDFrachel.avivNoch keine Bewertungen
- Halliburton, Just Some Spirits PDFDokument35 SeitenHalliburton, Just Some Spirits PDFrachel.avivNoch keine Bewertungen
- Hartnack, Vishnu On Freud's Desk PDFDokument30 SeitenHartnack, Vishnu On Freud's Desk PDFrachel.avivNoch keine Bewertungen
- Palozzi, Anorexia As Symptom of AffluentDokument7 SeitenPalozzi, Anorexia As Symptom of Affluentrachel.avivNoch keine Bewertungen
- Kleinman, Clinical Course of SZDokument13 SeitenKleinman, Clinical Course of SZrachel.avivNoch keine Bewertungen
- Kendler, The Nature of Psychiatric DisordersDokument8 SeitenKendler, The Nature of Psychiatric Disordersrachel.avivNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Kendler, The Nature of Psychiatric DisordersDokument8 SeitenKendler, The Nature of Psychiatric Disordersrachel.avivNoch keine Bewertungen
- Topic 8 Team LeadershipDokument45 SeitenTopic 8 Team Leadershipfariez79Noch keine Bewertungen
- Bedroom DesignDokument17 SeitenBedroom Designapi-292498910Noch keine Bewertungen
- 7 Principles of Software TestingDokument15 Seiten7 Principles of Software Testingsivachandran kaliappanNoch keine Bewertungen
- Pythagoras Project OutlineDokument2 SeitenPythagoras Project OutlineHillary Daniels Noch keine Bewertungen
- Recruitment and Selection Final ProjectDokument2 SeitenRecruitment and Selection Final ProjectFheikel DaudNoch keine Bewertungen
- FLOSS SS18 - Homework: Summary of Results and Research MethodsDokument1 SeiteFLOSS SS18 - Homework: Summary of Results and Research MethodsyyarenasNoch keine Bewertungen
- 1 Day Agile Essentials Refresher v1.2Dokument142 Seiten1 Day Agile Essentials Refresher v1.2pradeep6174Noch keine Bewertungen
- Physics Formula SheetDokument4 SeitenPhysics Formula Sheetraheemadom87Noch keine Bewertungen
- Behavioral Observation ChecklistDokument9 SeitenBehavioral Observation Checklistovidiu1159Noch keine Bewertungen
- B.Tech - Civil-SyllabusDokument126 SeitenB.Tech - Civil-SyllabusSrinivas JupalliNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- A Detailed Lesson Plan in EnglishDokument9 SeitenA Detailed Lesson Plan in EnglishElLa ElLaphotzx85% (13)
- IB SL AA Unit 13 Modelling Change More CalculusDokument7 SeitenIB SL AA Unit 13 Modelling Change More CalculusLorraine SabbaghNoch keine Bewertungen
- EAD-513 Cultural Functions in PracticeDokument2 SeitenEAD-513 Cultural Functions in PracticeKelly SchunkNoch keine Bewertungen
- Applied Mining Geology: Printed BookDokument1 SeiteApplied Mining Geology: Printed BookJavier CisnerosNoch keine Bewertungen
- Past Progressive Story 1 PDFDokument7 SeitenPast Progressive Story 1 PDFHafeed50% (8)
- Peplau's Theory of Interpersonal RelationsDokument24 SeitenPeplau's Theory of Interpersonal RelationsRN Samsan MasihNoch keine Bewertungen
- Pantech Software - NLP, ML, AI, Android, Big Data, Cloud Computing, NLP ProjectsDokument9 SeitenPantech Software - NLP, ML, AI, Android, Big Data, Cloud Computing, NLP ProjectsChandruNoch keine Bewertungen
- Can Digital Technology Change The Way Mathematics Skills Are Assessed?Dokument16 SeitenCan Digital Technology Change The Way Mathematics Skills Are Assessed?Erasmo IslasNoch keine Bewertungen
- SITXHRM010 Student Assessment Task 3Dokument9 SeitenSITXHRM010 Student Assessment Task 3Smile Reacts0% (1)
- Hodder Checkpoint Maths Spread PDFDokument9 SeitenHodder Checkpoint Maths Spread PDFswati0% (1)
- Study DesignsDokument24 SeitenStudy DesignsJasmen Sabroso PasiaNoch keine Bewertungen
- Test Bank For Cognition 7th Edition by RadvanskyDokument4 SeitenTest Bank For Cognition 7th Edition by RadvanskyJoel Studer100% (39)
- Final Udm Standard Syllabus - Social Work DocumentationDokument13 SeitenFinal Udm Standard Syllabus - Social Work DocumentationBenneth DasoNoch keine Bewertungen
- Lesson Plan Day 1Dokument5 SeitenLesson Plan Day 1api-313296159Noch keine Bewertungen
- Week 6 - Research MethodologyDokument26 SeitenWeek 6 - Research Methodologytaned8787Noch keine Bewertungen
- Soal Uts Bahasa Inggris Kelas 7Dokument3 SeitenSoal Uts Bahasa Inggris Kelas 7Mas Ruhan100% (1)
- Resume GerminDokument4 SeitenResume Germinlingesh1892Noch keine Bewertungen
- Guide For Taking and Scoring The ECCE Sample Test, Form BDokument3 SeitenGuide For Taking and Scoring The ECCE Sample Test, Form BRicardo PiguaveNoch keine Bewertungen
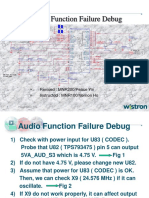
- Audio Function Failure DebugDokument11 SeitenAudio Function Failure Debugbeppino_andoNoch keine Bewertungen
- Week 5 FlowchartDokument1 SeiteWeek 5 FlowchartAlexNoch keine Bewertungen
- The Stoic Mindset: Living the Ten Principles of StoicismVon EverandThe Stoic Mindset: Living the Ten Principles of StoicismBewertung: 4.5 von 5 Sternen4.5/5 (10)
- The Power of Now: A Guide to Spiritual EnlightenmentVon EverandThe Power of Now: A Guide to Spiritual EnlightenmentBewertung: 4.5 von 5 Sternen4.5/5 (4125)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (28)
- Summary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesVon EverandSummary: Atomic Habits by James Clear: An Easy & Proven Way to Build Good Habits & Break Bad OnesBewertung: 5 von 5 Sternen5/5 (1635)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)