Das könnte Ihnen auch gefallen
- Celtic King de BountyDokument30 SeitenCeltic King de BountyLyubomir IvanovNoch keine Bewertungen
- Itish EnterpriseDokument46 SeitenItish EnterpriseCHEM PEACE100% (1)
- KWave ReportDokument8 SeitenKWave ReportDenys ShyshkinNoch keine Bewertungen
- MAIB - Collision Due To Anchor DragDokument16 SeitenMAIB - Collision Due To Anchor DragBinh Pham100% (1)
- Po Nedlloyd MagellanDokument44 SeitenPo Nedlloyd MagellanLyubomir IvanovNoch keine Bewertungen
- Accident Report: MV Spring Bok and MV Gas ArcticDokument12 SeitenAccident Report: MV Spring Bok and MV Gas Arcticlii liiNoch keine Bewertungen
- MV Willy: Report On The Investigation of The Grounding ofDokument33 SeitenMV Willy: Report On The Investigation of The Grounding ofLyubomir IvanovNoch keine Bewertungen
- Blue SinataDokument41 SeitenBlue SinataEd UrquizaNoch keine Bewertungen
- Collision Maersk Dover & Maersk VancouverDokument42 SeitenCollision Maersk Dover & Maersk VancouverMunteanu VictorNoch keine Bewertungen
- SExplorer DDalsoe02Dokument57 SeitenSExplorer DDalsoe02Lyubomir IvanovNoch keine Bewertungen
- Amenity Tor DaniaDokument36 SeitenAmenity Tor DaniaLyubomir IvanovNoch keine Bewertungen
- Dutch NavigatorDokument66 SeitenDutch NavigatorBinh Pham100% (1)
- AlexandraDokument52 SeitenAlexandraÇevik AhmetNoch keine Bewertungen
- 14 2020-04-SeatruckPerformanceDokument12 Seiten14 2020-04-SeatruckPerformanceJose Carlos RivaltaNoch keine Bewertungen
- MAIBReport Borga-1995Dokument39 SeitenMAIBReport Borga-1995Lyubomir IvanovNoch keine Bewertungen
- Wintertide and MSC Sabrina: Report On The Investigation The Collision BetweenDokument30 SeitenWintertide and MSC Sabrina: Report On The Investigation The Collision BetweenLyubomir IvanovNoch keine Bewertungen
- Rules of The Road: Case Study of The Collision Between MS Lykes Voyager and MS Washington SenatorDokument21 SeitenRules of The Road: Case Study of The Collision Between MS Lykes Voyager and MS Washington SenatorSidney BezerraNoch keine Bewertungen
- Risk Watch - Vol 19 No 2 - Jun 2012 PDFDokument8 SeitenRisk Watch - Vol 19 No 2 - Jun 2012 PDFkahl983100% (1)
- Eastfern KinsaleDokument30 SeitenEastfern KinsaleLyubomir IvanovNoch keine Bewertungen
- Marine Investigation Report M14P0014: Cap BlancheDokument18 SeitenMarine Investigation Report M14P0014: Cap BlancheLyubomir IvanovNoch keine Bewertungen
- Accident Report: Grounding of The Liquefied Gas Carrier On Haisborough Sand, North Sea 3 January 2014Dokument12 SeitenAccident Report: Grounding of The Liquefied Gas Carrier On Haisborough Sand, North Sea 3 January 2014IanmochaNoch keine Bewertungen
- Atlantic Mermaid and HampoelDokument36 SeitenAtlantic Mermaid and HampoelLyubomir IvanovNoch keine Bewertungen
- MAIBReport Cita 03 1998Dokument52 SeitenMAIBReport Cita 03 1998Haciane Mohamed FatehNoch keine Bewertungen
- Final RemakeDokument33 SeitenFinal RemakePrimo Ryan ZafeNoch keine Bewertungen
- Coastal Nav A1MC P1 - Catalogue of ErrorsDokument15 SeitenCoastal Nav A1MC P1 - Catalogue of Errorsnilakhan456790Noch keine Bewertungen
- 2009 Anchor Drag Young - LadyDokument57 Seiten2009 Anchor Drag Young - LadyAndrew WilliamsonNoch keine Bewertungen
- Navigation 2Dokument5 SeitenNavigation 2Nelum PereraNoch keine Bewertungen
- Grounding Case StudyDokument14 SeitenGrounding Case StudyRaghuNoch keine Bewertungen
- Risk Watch Vol 15 No 3Dokument8 SeitenRisk Watch Vol 15 No 3bogdanel_nba87100% (1)
- Ilovepdf MergedDokument10 SeitenIlovepdf MergedtimefdarkNoch keine Bewertungen
- Maritime Investigation Reveals A Litany of Errors and Neglect Resulting in Six FatalitiesDokument2 SeitenMaritime Investigation Reveals A Litany of Errors and Neglect Resulting in Six FatalitiesArn AmagnaNoch keine Bewertungen
- Timberland ReportDokument8 SeitenTimberland ReportfathanhaidarNoch keine Bewertungen
- Valentyn Yanivets 1492 Practical Work 5 Rules 9Dokument3 SeitenValentyn Yanivets 1492 Practical Work 5 Rules 9ReplаyMePleaseNoch keine Bewertungen
- Britishcygnet VeraDokument22 SeitenBritishcygnet VeraLyubomir IvanovNoch keine Bewertungen
- Safety Bulletin 3 2013Dokument4 SeitenSafety Bulletin 3 2013acmeaceNoch keine Bewertungen
- Nordsee and Poole SceneDokument26 SeitenNordsee and Poole SceneLyubomir IvanovNoch keine Bewertungen
- PaulaC DaryaGayatriDokument68 SeitenPaulaC DaryaGayatriDragos CalinNoch keine Bewertungen
- f1020 - Teamwork and LeadershipDokument13 Seitenf1020 - Teamwork and LeadershipAhmad Syarir AbdullahNoch keine Bewertungen
- Pentlan: An Investigation Into The Grounding of The Dry CarrierDokument21 SeitenPentlan: An Investigation Into The Grounding of The Dry CarrierLyubomir IvanovNoch keine Bewertungen
- Hoegh Osaka MAIB ReportDokument86 SeitenHoegh Osaka MAIB ReportIWCPOnlineNoch keine Bewertungen
- British Trent: The Investigation Into The Collision BetweenDokument42 SeitenBritish Trent: The Investigation Into The Collision BetweenLyubomir IvanovNoch keine Bewertungen
- Enak LoveletterDokument40 SeitenEnak LoveletterJohn CentenoNoch keine Bewertungen
- Jhon Raniel Acosta. Bsmt-Port Iii Marlaw Final Exam - : Human FactorDokument7 SeitenJhon Raniel Acosta. Bsmt-Port Iii Marlaw Final Exam - : Human FactorRnl AcstNoch keine Bewertungen
- Claude A DesgagnesDokument17 SeitenClaude A DesgagnesEmanuel HuardNoch keine Bewertungen
- Costa Concordia Case StudyDokument8 SeitenCosta Concordia Case StudyVinny CucciuffoNoch keine Bewertungen
- Isle of Man Ship Registry: CA99 - Scottish Bard and O Princess CollisionDokument50 SeitenIsle of Man Ship Registry: CA99 - Scottish Bard and O Princess CollisionLyubomir IvanovNoch keine Bewertungen
- Teslim 7664 20220401007 1671987766Dokument9 SeitenTeslim 7664 20220401007 1671987766timefdarkNoch keine Bewertungen
- Rencana Umum Kapal PenumpangDokument70 SeitenRencana Umum Kapal PenumpangFais HamzahNoch keine Bewertungen
- Viking Islay Confined Space Entry Accident PDFDokument46 SeitenViking Islay Confined Space Entry Accident PDFRauf HuseynovNoch keine Bewertungen
- Maritime Communications Case Study No7Dokument4 SeitenMaritime Communications Case Study No7Mickie DeWet100% (1)
- MIN 427 (M) : Lifejackets - Withdrawal of General Exemption To Carry Lifejackets On Class V Vessels On Inland LakesDokument3 SeitenMIN 427 (M) : Lifejackets - Withdrawal of General Exemption To Carry Lifejackets On Class V Vessels On Inland LakesvinayNoch keine Bewertungen
- A Test of SeamanshipDokument8 SeitenA Test of SeamanshipChristos Anthoulakis100% (1)
- Barfleur InteractionDokument16 SeitenBarfleur InteractionRabbitNoch keine Bewertungen
- MAIBReport QueenElizabeth2-1992Dokument34 SeitenMAIBReport QueenElizabeth2-1992Lyubomir IvanovNoch keine Bewertungen
- Particulars of The Vessel: Le Présent Rapport Est Également Disponible en FrançaisDokument23 SeitenParticulars of The Vessel: Le Présent Rapport Est Également Disponible en FrançaishgmNoch keine Bewertungen
- Casualty Report: Collision On 29 March 2001Dokument28 SeitenCasualty Report: Collision On 29 March 2001Lyubomir IvanovNoch keine Bewertungen
- Coastal Nav A1MC P1 - Catalogue of Errors 2016Dokument16 SeitenCoastal Nav A1MC P1 - Catalogue of Errors 2016nilakhan456790Noch keine Bewertungen
- Cypress: Beverley IIDokument30 SeitenCypress: Beverley IILyubomir IvanovNoch keine Bewertungen
- MetteeliasenukDokument18 SeitenMetteeliasenukLyubomir IvanovNoch keine Bewertungen
- FinalreportzeranogtosteDokument23 SeitenFinalreportzeranogtosteLyubomir IvanovNoch keine Bewertungen
- Nedlloyd Vespucci and WahkunaDokument58 SeitenNedlloyd Vespucci and WahkunaLyubomir IvanovNoch keine Bewertungen
- New Flame Report - 105827aDokument34 SeitenNew Flame Report - 105827aLyubomir IvanovNoch keine Bewertungen
- Klazina VeraDokument12 SeitenKlazina VeraLyubomir IvanovNoch keine Bewertungen
- Hoorobin and Arklow MarshDokument24 SeitenHoorobin and Arklow MarshLyubomir IvanovNoch keine Bewertungen
- Lykes VoyagerDokument44 SeitenLykes VoyagerAli MovagharNoch keine Bewertungen
- Wilhelmina J: of ofDokument49 SeitenWilhelmina J: of ofLyubomir IvanovNoch keine Bewertungen
- Cypress: Beverley IIDokument30 SeitenCypress: Beverley IILyubomir IvanovNoch keine Bewertungen
- Ash and Dutch AquamarineDokument44 SeitenAsh and Dutch AquamarineSebastian Ionut TanaseNoch keine Bewertungen
- Arctic Ocean-Maritime LadyDokument66 SeitenArctic Ocean-Maritime LadysbdmanNoch keine Bewertungen
- GULDBORGDokument10 SeitenGULDBORGLyubomir IvanovNoch keine Bewertungen
- Audacity Leonis ReportDokument44 SeitenAudacity Leonis ReportLyubomir IvanovNoch keine Bewertungen
- Casualty Report: Collision On 29 March 2001Dokument28 SeitenCasualty Report: Collision On 29 March 2001Lyubomir IvanovNoch keine Bewertungen
- Wintertide and MSC Sabrina: Report On The Investigation The Collision BetweenDokument30 SeitenWintertide and MSC Sabrina: Report On The Investigation The Collision BetweenLyubomir IvanovNoch keine Bewertungen
- KRASLAVA and ATLANTIC LADY - Collision On 1 November 2014Dokument28 SeitenKRASLAVA and ATLANTIC LADY - Collision On 1 November 2014Lyubomir IvanovNoch keine Bewertungen
- British Trent: The Investigation Into The Collision BetweenDokument42 SeitenBritish Trent: The Investigation Into The Collision BetweenLyubomir IvanovNoch keine Bewertungen
- Spring Glory Josephine Maersk 2012Dokument29 SeitenSpring Glory Josephine Maersk 2012Viorel Andrei100% (2)
- Pasadena Universal Nordheim06Dokument31 SeitenPasadena Universal Nordheim06Lyubomir IvanovNoch keine Bewertungen
- SExplorer DDalsoe02Dokument57 SeitenSExplorer DDalsoe02Lyubomir IvanovNoch keine Bewertungen
- Frank W Lilly Engelsk FiskDokument14 SeitenFrank W Lilly Engelsk FiskLyubomir IvanovNoch keine Bewertungen
- Gotland Carolina / Conti Harmony Collision On 19 April 2008Dokument17 SeitenGotland Carolina / Conti Harmony Collision On 19 April 2008Lyubomir IvanovNoch keine Bewertungen
- Gudermes Saint JacquesDokument35 SeitenGudermes Saint JacquesLyubomir IvanovNoch keine Bewertungen
- Homeland: Report No 4/2011 March 2011Dokument38 SeitenHomeland: Report No 4/2011 March 2011Lyubomir IvanovNoch keine Bewertungen
- Cepheus J-IleksaDokument41 SeitenCepheus J-IleksaLyubomir IvanovNoch keine Bewertungen
- FU Shan Hai gdnyniaNO3Dokument33 SeitenFU Shan Hai gdnyniaNO3Lyubomir IvanovNoch keine Bewertungen
- ACXHibiscus-HyundaiDiscovery AnnexesDokument82 SeitenACXHibiscus-HyundaiDiscovery AnnexesLyubomir IvanovNoch keine Bewertungen
- Atlantic Mermaid and HampoelDokument36 SeitenAtlantic Mermaid and HampoelLyubomir IvanovNoch keine Bewertungen
- BergittaandeyraDokument30 SeitenBergittaandeyraLyubomir IvanovNoch keine Bewertungen
- Motor Boats & Launch CatalogueDokument98 SeitenMotor Boats & Launch CatalogueDeganchileNoch keine Bewertungen
- w1 c26 2Dokument3 Seitenw1 c26 2api-205480101Noch keine Bewertungen
- Diagrama Eléctrico Caterpillar 3406E PDFDokument2 SeitenDiagrama Eléctrico Caterpillar 3406E PDFDavid.Quijano100% (3)
- Siemens PLM NX Automotive Packaging Fs 68168 A3 - tcm27 29307Dokument5 SeitenSiemens PLM NX Automotive Packaging Fs 68168 A3 - tcm27 29307SoumenAtaNoch keine Bewertungen
- Surface Vehicle Standard: Issued JUL97Dokument19 SeitenSurface Vehicle Standard: Issued JUL97anupthattaNoch keine Bewertungen
- P66 XC Aviation Hydraulic Oil SDSDokument8 SeitenP66 XC Aviation Hydraulic Oil SDSMik AeilNoch keine Bewertungen
- Build SheetDokument5 SeitenBuild SheetcoreyNoch keine Bewertungen
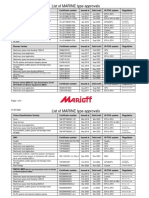
- Marioff 2021 07 01 EN Approval Matrix Marine Table - tcm986 148336Dokument4 SeitenMarioff 2021 07 01 EN Approval Matrix Marine Table - tcm986 148336Pavel DrugakovNoch keine Bewertungen
- Terex BT3470Dokument4 SeitenTerex BT3470Ari Gabriel Sanchez GarciaNoch keine Bewertungen
- AP-T200-12 Bridge Design Guidelines For EQDokument133 SeitenAP-T200-12 Bridge Design Guidelines For EQRasiduzzaman RashidNoch keine Bewertungen
- SMRT Annual Report 2016Dokument141 SeitenSMRT Annual Report 2016Sassy TanNoch keine Bewertungen
- Eta 02 03Dokument26 SeitenEta 02 03Miyanda HimachilaNoch keine Bewertungen
- Klijn&Scholten - Delft Central - 2015Dokument9 SeitenKlijn&Scholten - Delft Central - 2015vnchr.kNoch keine Bewertungen
- Pot Bearings Technical Data Sheets All Standards PDFDokument30 SeitenPot Bearings Technical Data Sheets All Standards PDFStefanoPalumboNoch keine Bewertungen
- Aditya Joshi CVDokument23 SeitenAditya Joshi CVAditya JoshiNoch keine Bewertungen
- Merlo DBM 2000 2500 3500 en PDFDokument8 SeitenMerlo DBM 2000 2500 3500 en PDFJozef50% (4)
- Managing Airport Construction ProjectsDokument10 SeitenManaging Airport Construction ProjectsTATATAHER100% (1)
- HM 40 Feb 2023 Edi, Cow, EditableDokument36 SeitenHM 40 Feb 2023 Edi, Cow, EditableAung Htet KyawNoch keine Bewertungen
- 18.1 X Bar S Chart SheetDokument10 Seiten18.1 X Bar S Chart SheetSaurav KumarNoch keine Bewertungen
- Northwest African Air Forces-1943Dokument39 SeitenNorthwest African Air Forces-1943cjnjr1Noch keine Bewertungen
- Capital Strutur of FMCG &automobile SectorDokument39 SeitenCapital Strutur of FMCG &automobile SectorJithin PonathilNoch keine Bewertungen
- West Tower vs. Phil. Ind. Corp.Dokument14 SeitenWest Tower vs. Phil. Ind. Corp.Antonio Dominic SalvadorNoch keine Bewertungen
- Iit BombayDokument3 SeitenIit BombayAakanksha ParasharNoch keine Bewertungen
- Rockefeller - A Richest Man Ever !!Dokument8 SeitenRockefeller - A Richest Man Ever !!kartikey SharmaNoch keine Bewertungen
- Railway Equipment 1004-En LowresDokument15 SeitenRailway Equipment 1004-En LowresSivaneswaran SabaratnamNoch keine Bewertungen
- Piese VW SwagDokument377 SeitenPiese VW SwagIon OlteanuNoch keine Bewertungen
- Agreement: /ECE/324/Rev.2/Add.129 /ECE/TRANS/505/Rev.2/Add.129Dokument25 SeitenAgreement: /ECE/324/Rev.2/Add.129 /ECE/TRANS/505/Rev.2/Add.129László KovácsNoch keine Bewertungen
- Carspotting: The Real Adventures of Irvine Welsh by Sandy MacnairDokument40 SeitenCarspotting: The Real Adventures of Irvine Welsh by Sandy MacnairBlack & White Publishing100% (1)
- Aga Khan Walk CritiqueDokument21 SeitenAga Khan Walk CritiqueMaisieNoch keine Bewertungen
- Dr. San Htin Lin - APOST FESS Workshop - Final Info PackageDokument6 SeitenDr. San Htin Lin - APOST FESS Workshop - Final Info PackageHtin Lin SanNoch keine Bewertungen