Das könnte Ihnen auch gefallen
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Respiratory Distress SyndromeDokument41 SeitenRespiratory Distress Syndromef.abrahamNoch keine Bewertungen
- Nursing the NeonateVon EverandNursing the NeonateMaggie MeeksNoch keine Bewertungen
- Acynotic Heart DiseasesDokument13 SeitenAcynotic Heart DiseasesSimran JosanNoch keine Bewertungen
- Acynotic DiseaseDokument55 SeitenAcynotic DiseaseTesfamichael AbathunNoch keine Bewertungen
- Neonatal Hypoglycemia (Infant of Diabetic Mother)Dokument15 SeitenNeonatal Hypoglycemia (Infant of Diabetic Mother)diana rossNoch keine Bewertungen
- Congenital Heart Disease - ASDDokument36 SeitenCongenital Heart Disease - ASDAuni Akif Aleesa100% (1)
- Renal Failure in ChildrenDokument43 SeitenRenal Failure in Childrendennyyy175Noch keine Bewertungen
- 4 Meconium Aspiration SyndromeDokument30 Seiten4 Meconium Aspiration SyndromeRana Vandana100% (2)
- Respiratory Distress SyndromeDokument30 SeitenRespiratory Distress SyndromeDennis MiritiNoch keine Bewertungen
- Acute Respiratory Distress SyndromeDokument3 SeitenAcute Respiratory Distress Syndromekarenkaren09Noch keine Bewertungen
- Dyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDokument19 SeitenDyspnea: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafNoch keine Bewertungen
- Adrenal CrisisDokument6 SeitenAdrenal CrisisSteven SetioNoch keine Bewertungen
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDokument23 SeitenAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaNoch keine Bewertungen
- Tetralogy of FallotDokument10 SeitenTetralogy of FallotanggiehardiyantiNoch keine Bewertungen
- Peritonel DialysisDokument8 SeitenPeritonel DialysisSudesh TomarNoch keine Bewertungen
- Acute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) NovemberDokument28 SeitenAcute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) Novemberزكريا عمرNoch keine Bewertungen
- Lecture Notes On AphDokument41 SeitenLecture Notes On AphEyob MizanNoch keine Bewertungen
- Hypospadias and Epispadias 1Dokument35 SeitenHypospadias and Epispadias 1Corey100% (1)
- Pediatric Liver TransplantationDokument30 SeitenPediatric Liver TransplantationMadhu Sinha100% (1)
- AsphyxiaDokument35 SeitenAsphyxiaAna Cristina Montillano100% (1)
- Hypoxic Ischemic EncephalopathyDokument7 SeitenHypoxic Ischemic EncephalopathyJennesse May Guiao IbayNoch keine Bewertungen
- Maternal and Child Health Programmes AssignmentDokument11 SeitenMaternal and Child Health Programmes Assignmentannu panchal80% (5)
- Rheumatic Fever and RHDDokument49 SeitenRheumatic Fever and RHDbereket gashuNoch keine Bewertungen
- Lymphoma in ChildrenDokument42 SeitenLymphoma in ChildrenPriyaNoch keine Bewertungen
- Neonatal Heart DiseaseDokument8 SeitenNeonatal Heart DiseaseDelphy VargheseNoch keine Bewertungen
- Neonatal ResuscitationDokument15 SeitenNeonatal ResuscitationAmruta GadeNoch keine Bewertungen
- Acute Renal FailureDokument25 SeitenAcute Renal FailureRyan Akhmad Adhi SaputraNoch keine Bewertungen
- Bag Mask VentilationDokument35 SeitenBag Mask VentilationedrinsneNoch keine Bewertungen
- Heart Disease in Pregnancy: Mohana PreeshaDokument50 SeitenHeart Disease in Pregnancy: Mohana PreeshaChuks LeviNoch keine Bewertungen
- Fetal CirculationDokument13 SeitenFetal CirculationPraveen YadavNoch keine Bewertungen
- Pediatrics Intensive Care Unit: Presented By: Ms. Sandeep KaurDokument52 SeitenPediatrics Intensive Care Unit: Presented By: Ms. Sandeep KaurArchanaNoch keine Bewertungen
- CLINICAL PRESENTATION ON IugrDokument24 SeitenCLINICAL PRESENTATION ON Iugrsaleha sultanaNoch keine Bewertungen
- Birth AsphyxiaDokument10 SeitenBirth Asphyxiasarita Singh MaharjanNoch keine Bewertungen
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDokument12 SeitenMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNoch keine Bewertungen
- Poisoning in ChildrenDokument46 SeitenPoisoning in ChildrenPooja ChapdiNoch keine Bewertungen
- Hypertrophic Pyloric StenosisDokument23 SeitenHypertrophic Pyloric StenosisRahel Imelda PanggabeanNoch keine Bewertungen
- Asphyxia NeonatorumDokument35 SeitenAsphyxia NeonatorumMuhammad RagilNoch keine Bewertungen
- Nursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDokument26 SeitenNursing Care of Children With Indian Childhood Cirrhosis, Wilsons Disesase, Reyes SyndromeDivya Nair100% (2)
- Failure To ThriveDokument4 SeitenFailure To ThriveShane PangilinanNoch keine Bewertungen
- Respiratory Disorder Note BSC 3rd YearDokument41 SeitenRespiratory Disorder Note BSC 3rd YearNancyNoch keine Bewertungen
- 16 Amniotic Fluid EmbolismDokument46 Seiten16 Amniotic Fluid EmbolismAhmed TarigNoch keine Bewertungen
- Disorders of Skin in ChildrenDokument47 SeitenDisorders of Skin in Childrensmriti boraNoch keine Bewertungen
- Presentation On Current Principles and Practices of Pediatric NursingDokument18 SeitenPresentation On Current Principles and Practices of Pediatric Nursingmalleshwari athramNoch keine Bewertungen
- Abnormal LabourDokument7 SeitenAbnormal LabourSaman SarKo0% (1)
- Fetal CirculationDokument2 SeitenFetal CirculationgoldiemareNoch keine Bewertungen
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDokument31 SeitenPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNoch keine Bewertungen
- Seminar 2 Endocrine DisordersDokument44 SeitenSeminar 2 Endocrine DisordersSuganthi ParthibanNoch keine Bewertungen
- Neonatal SepsisDokument63 SeitenNeonatal SepsisDemewoz Fikir100% (2)
- Introduction To Pediatric NursingDokument36 SeitenIntroduction To Pediatric Nursingcharan poonia100% (1)
- 5 Bleeding Disorders PPT EditedDokument87 Seiten5 Bleeding Disorders PPT EditedFrances Isabella OlasimanNoch keine Bewertungen
- Meconium Aspiration Syndrome (MAS)Dokument12 SeitenMeconium Aspiration Syndrome (MAS)Angela AmaoNoch keine Bewertungen
- Pyloric StenosisDokument3 SeitenPyloric Stenosismagisasamundo100% (1)
- HemophiliaDokument20 SeitenHemophiliaNavirohit GillNoch keine Bewertungen
- Pediatric Asthma ScoreDokument1 SeitePediatric Asthma ScoreMumunni MoretzNoch keine Bewertungen
- Fetal Distress Day 1Dokument16 SeitenFetal Distress Day 1Bharat ThapaNoch keine Bewertungen
- Teaching Module Hypertension PregnancyDokument17 SeitenTeaching Module Hypertension PregnancyQueenie BlasurcaNoch keine Bewertungen
- Congenital Heart DiseaseDokument43 SeitenCongenital Heart DiseaseSalman Majid100% (1)
- Management of Neonatal HypoglycemiaDokument14 SeitenManagement of Neonatal Hypoglycemiaece142Noch keine Bewertungen
- Patient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDokument93 SeitenPatient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDay MedsNoch keine Bewertungen
- Nursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearDokument34 SeitenNursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearSimran JosanNoch keine Bewertungen
- Orlando's TheoryDokument52 SeitenOrlando's TheorySimran Josan100% (1)
- Curriculum FOR B.Sc. Nursing CourseDokument133 SeitenCurriculum FOR B.Sc. Nursing Coursesimonjosan100% (1)
- FEVERDokument8 SeitenFEVERSimran JosanNoch keine Bewertungen
- Orem'S Self-Care Deficit TheoryDokument52 SeitenOrem'S Self-Care Deficit TheorySimran JosanNoch keine Bewertungen
- Orem's Theory ApplicationDokument45 SeitenOrem's Theory ApplicationSimran JosanNoch keine Bewertungen
- Course of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsDokument3 SeitenCourse of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsSimran JosanNoch keine Bewertungen
- Medical AsepsisDokument9 SeitenMedical AsepsisSimran JosanNoch keine Bewertungen
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnDokument7 SeitenCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- SUBMITTED TO - Resp. Mr. Somorjit SinghDokument8 SeitenSUBMITTED TO - Resp. Mr. Somorjit SinghSimran JosanNoch keine Bewertungen
- ENDOTRACHEAL INTUBATIOn SandeepDokument17 SeitenENDOTRACHEAL INTUBATIOn SandeepSimran JosanNoch keine Bewertungen
- CARDIAC Invasive Procedures FinalDokument19 SeitenCARDIAC Invasive Procedures FinalSimran JosanNoch keine Bewertungen
- Arterial Blood Gas Analysis PROCEDUREDokument6 SeitenArterial Blood Gas Analysis PROCEDURESimran Josan100% (4)
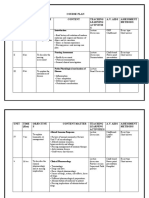
- Course Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsDokument8 SeitenCourse Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsSimran JosanNoch keine Bewertungen
- Cardiac Diagnostic TestsDokument14 SeitenCardiac Diagnostic TestsSimran Josan100% (5)
- Unit Plan: Unit TIME (HRS) Objective S Content Teaching Learning Activities A.V. Aids Assessment MethodsDokument2 SeitenUnit Plan: Unit TIME (HRS) Objective S Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan63% (8)
- Unit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsDokument4 SeitenUnit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan100% (1)
- Anatomy and Physiology of Colon of Case StudyDokument4 SeitenAnatomy and Physiology of Colon of Case StudySimran JosanNoch keine Bewertungen
- Cardiac Surgery and InvestigationDokument30 SeitenCardiac Surgery and InvestigationSimran JosanNoch keine Bewertungen
- LESSON PLAN ON CommunicationDokument11 SeitenLESSON PLAN ON CommunicationSimran Josan100% (6)
- Anatomy and Physiology of Nervous SystemDokument13 SeitenAnatomy and Physiology of Nervous SystemSimran JosanNoch keine Bewertungen
- Unit Plan MSC 1 FRST Year - Docx 22Dokument5 SeitenUnit Plan MSC 1 FRST Year - Docx 22Simran JosanNoch keine Bewertungen
- Anatomy and Physiology of HeartDokument2 SeitenAnatomy and Physiology of HeartSimran JosanNoch keine Bewertungen
- Disease Condition of MastectomyDokument5 SeitenDisease Condition of MastectomySimran JosanNoch keine Bewertungen
- Disease Condition of MastectomyDokument5 SeitenDisease Condition of MastectomySimran JosanNoch keine Bewertungen
- Disease Condition... Diabetes MellitusDokument6 SeitenDisease Condition... Diabetes MellitusSimran JosanNoch keine Bewertungen
- Complete FractureDokument10 SeitenComplete FractureSimran JosanNoch keine Bewertungen
- Disease Condition of ColonDokument4 SeitenDisease Condition of ColonSimran JosanNoch keine Bewertungen
- Parameters Identification of Induction Motor Model BasedDokument10 SeitenParameters Identification of Induction Motor Model Basedretrueke1170Noch keine Bewertungen
- Vanish Magic Magazine VANISH MAGIC MAGAZINE 58 May 2019Dokument118 SeitenVanish Magic Magazine VANISH MAGIC MAGAZINE 58 May 2019mick byrnes100% (1)
- Multi Pressure Refrigeration CyclesDokument41 SeitenMulti Pressure Refrigeration CyclesSyed Wajih Ul Hassan80% (10)
- Ict 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Dokument14 SeitenIct 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Chiropractic Marketing NowNoch keine Bewertungen
- LinkageDokument9 SeitenLinkageHarshu JunghareNoch keine Bewertungen
- Dharmakirti39s Commentary On ChakrasamvaraDokument15 SeitenDharmakirti39s Commentary On ChakrasamvaraThiago AlbuquerqueNoch keine Bewertungen
- Statics: Vector Mechanics For EngineersDokument39 SeitenStatics: Vector Mechanics For EngineersVijay KumarNoch keine Bewertungen
- 2nd APJ Abdul Kalam Essay Writing CompetitionDokument2 Seiten2nd APJ Abdul Kalam Essay Writing CompetitionANURAG SINGHNoch keine Bewertungen
- Usp Description and SolubilityDokument1 SeiteUsp Description and SolubilityvafaashkNoch keine Bewertungen
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDokument2 SeitenRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNoch keine Bewertungen
- GSD Puppy Training Essentials PDFDokument2 SeitenGSD Puppy Training Essentials PDFseja saulNoch keine Bewertungen
- Yoga SadhguruDokument6 SeitenYoga Sadhgurucosti.sorescuNoch keine Bewertungen
- Ecall Vs NG EcallDokument6 SeitenEcall Vs NG EcallTrần Văn DũngNoch keine Bewertungen
- Coffee Quality Manual by Abra Rand Nig Use IDokument25 SeitenCoffee Quality Manual by Abra Rand Nig Use IIpungNoch keine Bewertungen
- Presentation AcetanilideDokument22 SeitenPresentation AcetanilideNovitasarii JufriNoch keine Bewertungen
- Gaffin, Biblical Theology and Westminster StandardsDokument16 SeitenGaffin, Biblical Theology and Westminster StandardstheoarticlesNoch keine Bewertungen
- Electronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMDokument2 SeitenElectronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMNesha Siva Shanmugam ShavannahNoch keine Bewertungen
- Book Index The Art of Heavy TransportDokument6 SeitenBook Index The Art of Heavy TransportHermon Pakpahan50% (2)
- AIR Conditioner: Owner'S ManualDokument52 SeitenAIR Conditioner: Owner'S Manualashley diazNoch keine Bewertungen
- Eco Exercise 3answer Ans 1Dokument8 SeitenEco Exercise 3answer Ans 1Glory PrintingNoch keine Bewertungen
- Ap, Lrrsisal of Roentgenograph, Ic: I SsayDokument30 SeitenAp, Lrrsisal of Roentgenograph, Ic: I SsayMindaugasStacevičiusNoch keine Bewertungen
- SR No Service CodeDokument30 SeitenSR No Service CodeShiva KrishnaNoch keine Bewertungen
- Types of Loads Considered For Design of BridgeDokument45 SeitenTypes of Loads Considered For Design of BridgeAbhishek100% (1)
- Clinical Biomechanics: Leigh W. Marshall, Stuart M. McgillDokument4 SeitenClinical Biomechanics: Leigh W. Marshall, Stuart M. McgillMichael JunNoch keine Bewertungen
- Prevailing Torque Locknut Technical SpecificationsDokument3 SeitenPrevailing Torque Locknut Technical SpecificationsLiu YangtzeNoch keine Bewertungen
- EXCEL For Pump DesignDokument2 SeitenEXCEL For Pump Designkad-7Noch keine Bewertungen
- Armadio Presentation-2019Dokument45 SeitenArmadio Presentation-2019Subhash Singh TomarNoch keine Bewertungen
- Designing and Building A Computer TableDokument9 SeitenDesigning and Building A Computer Tablemaster_codersNoch keine Bewertungen
- Karl MarxDokument4 SeitenKarl Marxeirvine noah isidroNoch keine Bewertungen
- Chapter 7 Dopant Diffusion - IDokument32 SeitenChapter 7 Dopant Diffusion - I강준호Noch keine Bewertungen
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (3)
- Gut: the new and revised Sunday Times bestsellerVon EverandGut: the new and revised Sunday Times bestsellerBewertung: 4 von 5 Sternen4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningVon EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningBewertung: 4 von 5 Sternen4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- An Autobiography of Trauma: A Healing JourneyVon EverandAn Autobiography of Trauma: A Healing JourneyBewertung: 5 von 5 Sternen5/5 (2)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)