Das könnte Ihnen auch gefallen
- Parvo Virus CureDokument1 SeiteParvo Virus CureNoel IV T. BorromeoNoch keine Bewertungen
- Year: Not Applicable: I. Major OperationsDokument5 SeitenYear: Not Applicable: I. Major Operationsayhab abinaNoch keine Bewertungen
- The Philippine Cancer Control ProgramDokument10 SeitenThe Philippine Cancer Control ProgramJohnryl FranciscoNoch keine Bewertungen
- Letter of ConsiderationDokument1 SeiteLetter of ConsiderationNick CorrosivesnareNoch keine Bewertungen
- Contract Agreement Modular CabinetsDokument5 SeitenContract Agreement Modular CabinetsVon Joby RomeroNoch keine Bewertungen
- ASMPH PRIMAN Syllabus Revised July 2017Dokument20 SeitenASMPH PRIMAN Syllabus Revised July 2017JHENNE KYLE DEENoch keine Bewertungen
- Philhealth cf4Dokument6 SeitenPhilhealth cf4Jose AcuinNoch keine Bewertungen
- Ospital NG Maynila Medical Center: Department of SURGERYDokument4 SeitenOspital NG Maynila Medical Center: Department of SURGERYPM Basiloy - AloNoch keine Bewertungen
- Basic Math Ability Exam A Relias Graded ADokument6 SeitenBasic Math Ability Exam A Relias Graded ADebs MaxNoch keine Bewertungen
- Student Excursion Consent FormDokument4 SeitenStudent Excursion Consent Formapi-276186998Noch keine Bewertungen
- Swot AnalysisDokument3 SeitenSwot AnalysisMay Lj33% (3)
- Memorandum of Agreement BCJDokument5 SeitenMemorandum of Agreement BCJReinald Raven GuerreroNoch keine Bewertungen
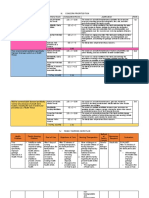
- Iii. Concern Prioritization Health Concern Criteria/ Scale Computation/Score Justification RankDokument3 SeitenIii. Concern Prioritization Health Concern Criteria/ Scale Computation/Score Justification RankKae MacalinaoNoch keine Bewertungen
- Mantilla-Neil, EssayDokument7 SeitenMantilla-Neil, EssayJohn ManaloNoch keine Bewertungen
- Vehicular Accident KimantongDokument3 SeitenVehicular Accident KimantongAngel MangaNoch keine Bewertungen
- Initial Plan of Activities CHN PCIDokument1 SeiteInitial Plan of Activities CHN PCIJaidelo MagallonNoch keine Bewertungen
- Makati Medical CenterDokument2 SeitenMakati Medical CenterDaniel Vergara ArceNoch keine Bewertungen
- IV Fluids and Blood Products-No d5nrDokument13 SeitenIV Fluids and Blood Products-No d5nrMeriz PorcaNoch keine Bewertungen
- Useful Bisaya (Cebuano) Phrases When Visiting Visayas and MindanaoDokument9 SeitenUseful Bisaya (Cebuano) Phrases When Visiting Visayas and MindanaoSchuldich SchwarzNoch keine Bewertungen
- Nurs1121 PosDokument17 SeitenNurs1121 PosRapplerNoch keine Bewertungen
- Gonzales Zosimo AbstractDokument2 SeitenGonzales Zosimo AbstractDarnel Jasper HurtadoNoch keine Bewertungen
- FCM3-3.03 Renal Disease Control ProgramDokument10 SeitenFCM3-3.03 Renal Disease Control ProgramJoher MendezNoch keine Bewertungen
- PRC Case FormDokument5 SeitenPRC Case FormiamELHIZANoch keine Bewertungen
- DO 2013-0100 DOH NCP Operational GuidelinesDokument6 SeitenDO 2013-0100 DOH NCP Operational GuidelinesHarby Ongbay AbellanosaNoch keine Bewertungen
- Q A 1Dokument48 SeitenQ A 1ChannelGNoch keine Bewertungen
- Know All Men by These Presents:: Lease ContractDokument3 SeitenKnow All Men by These Presents:: Lease ContractRainnie McBeeNoch keine Bewertungen
- MCI Drill Sample ScenariosDokument8 SeitenMCI Drill Sample ScenariosDarylNoch keine Bewertungen
- CPH FORM 2 - Common Household QuestionnaireDokument6 SeitenCPH FORM 2 - Common Household Questionnairebanate LGU100% (1)
- Vision Mission MCPDokument2 SeitenVision Mission MCPgerald_ichigoNoch keine Bewertungen
- DM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Dokument55 SeitenDM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Seriel TismoNoch keine Bewertungen
- MDlist 2017 NORTH YudelDokument15 SeitenMDlist 2017 NORTH YudelericNoch keine Bewertungen
- Professional Development PlanDokument2 SeitenProfessional Development Planapi-578003485Noch keine Bewertungen
- Affidavit of Loss TOPDokument2 SeitenAffidavit of Loss TOPJM CamalonNoch keine Bewertungen
- HTP DM ParesisDokument4 SeitenHTP DM ParesisTami GemarinoNoch keine Bewertungen
- Profile AmpucaoDokument28 SeitenProfile Ampucaotonton ton100% (1)
- Letter of ApologyDokument1 SeiteLetter of ApologyDorobantu DragosNoch keine Bewertungen
- Fecalysis SampleDokument1 SeiteFecalysis SampleReiel PeñaNoch keine Bewertungen
- Vildagliptin + Metformin (Eucreas) PDFDokument19 SeitenVildagliptin + Metformin (Eucreas) PDFddandan_2Noch keine Bewertungen
- New - WAIVER AND RELEASE FROM LIABILITYDokument1 SeiteNew - WAIVER AND RELEASE FROM LIABILITYralph tuba-onNoch keine Bewertungen
- Informed Consent (English & Filipino)Dokument2 SeitenInformed Consent (English & Filipino)Angelica Anne ReyNoch keine Bewertungen
- Test Questions CA1Dokument3 SeitenTest Questions CA1Gemery Jade ArtatesNoch keine Bewertungen
- Sample Hematology ResultDokument3 SeitenSample Hematology ResultRaul ArranguezNoch keine Bewertungen
- Guidelines Implementing Rle: Based On CHED MEMORANDUM ORDER 14 Series of 2009Dokument43 SeitenGuidelines Implementing Rle: Based On CHED MEMORANDUM ORDER 14 Series of 2009Ameng GosimNoch keine Bewertungen
- ITRMC Vision and MissionDokument1 SeiteITRMC Vision and MissionDeniseNoch keine Bewertungen
- Doh2011 2013isspDokument191 SeitenDoh2011 2013isspJay Pee CruzNoch keine Bewertungen
- Cover LetterDokument2 SeitenCover Letterapi-533999698Noch keine Bewertungen
- Ched Scholarship Unifast Tertiary Education Subsidy (Tes) : Olfu College of NursingDokument3 SeitenChed Scholarship Unifast Tertiary Education Subsidy (Tes) : Olfu College of Nursingsorry important businesseuNoch keine Bewertungen
- PWD Center OrdinanceDokument4 SeitenPWD Center OrdinanceIrish Dale Louise M. DimitimanNoch keine Bewertungen
- BSN 3 3 - Group 5 - Lived Experiences of Filipino Family Members Who Signed A Do Not Resuscitate ContractDokument19 SeitenBSN 3 3 - Group 5 - Lived Experiences of Filipino Family Members Who Signed A Do Not Resuscitate ContractJan Charlie SophiaNoch keine Bewertungen
- St. Paul University Dumaguete College of Nursing S. Y. 2011-2012Dokument7 SeitenSt. Paul University Dumaguete College of Nursing S. Y. 2011-2012anne_valencia_3Noch keine Bewertungen
- Authorization LetterDokument1 SeiteAuthorization LetterRaeinhyer JohnNoch keine Bewertungen
- TB and LeprosyDokument39 SeitenTB and LeprosyCharise Ligores100% (1)
- Patient's ProfileDokument4 SeitenPatient's ProfileSnowhite NeymarNoch keine Bewertungen
- Reflection About The Make Up ClassDokument1 SeiteReflection About The Make Up Classnikol crisang100% (1)
- Certification: Department of Health/Rural Health UnitDokument3 SeitenCertification: Department of Health/Rural Health UnitgeshaNoch keine Bewertungen
- Senior Citizen PointersDokument3 SeitenSenior Citizen PointersDino MacavintaNoch keine Bewertungen
- dm2019-0365 Interim Guidelines On LNS SQDokument8 Seitendm2019-0365 Interim Guidelines On LNS SQMary Joy GaloloNoch keine Bewertungen
- Case Study FormatDokument5 SeitenCase Study FormatEden OlasabNoch keine Bewertungen
- NVS Written ReportDokument20 SeitenNVS Written ReportbabiNoch keine Bewertungen
- OsteoarthritisDokument10 SeitenOsteoarthritisRehanNoch keine Bewertungen
- Evaluation and FHSISDokument6 SeitenEvaluation and FHSISShara SampangNoch keine Bewertungen
- Drug StudyDokument7 SeitenDrug StudyArnel MacabalitaoNoch keine Bewertungen
- Comorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dokument10 SeitenComorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dini AgustiniNoch keine Bewertungen
- Nurse Shift PDFDokument11 SeitenNurse Shift PDFWisnu YogaNoch keine Bewertungen
- Teaching Plan SampleDokument3 SeitenTeaching Plan SampleSoleil MaxwellNoch keine Bewertungen
- Terms and Strategies For Medical RecordsDokument7 SeitenTerms and Strategies For Medical RecordsNaysha RomeroNoch keine Bewertungen
- PNC Checklist AfricanDokument2 SeitenPNC Checklist AfricanAudrey Andini0% (1)
- Mental IllnessDokument3 SeitenMental IllnessKate EvangelistaNoch keine Bewertungen
- PhobiaDokument4 SeitenPhobiaZeba QuadiriNoch keine Bewertungen
- Venous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesDokument13 SeitenVenous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesSebastiano Della CasaNoch keine Bewertungen
- IDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFDokument152 SeitenIDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFVivek KhakharNoch keine Bewertungen
- Using Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSDokument2 SeitenUsing Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSSevina Eka ChannelNoch keine Bewertungen
- Medical Symptoms QuestionnaireDokument29 SeitenMedical Symptoms QuestionnaireOlesiaNoch keine Bewertungen
- Imle 18.02.2013Dokument47 SeitenImle 18.02.2013Nas Man100% (1)
- Acute Gastritis CiciDokument43 SeitenAcute Gastritis CiciDwi Rezky AmaliaNoch keine Bewertungen
- Insulin SensitizersDokument17 SeitenInsulin SensitizersGautam SharmaNoch keine Bewertungen
- Case Study 5 Dengue Fever CorrectedDokument13 SeitenCase Study 5 Dengue Fever CorrectedyounggirldavidNoch keine Bewertungen
- Proximal Humerus Fractures Epidemiology and TrendsDokument5 SeitenProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesNoch keine Bewertungen
- Anxiety: What Are Some Symptoms of Anxiety?Dokument3 SeitenAnxiety: What Are Some Symptoms of Anxiety?Khairil AshrafNoch keine Bewertungen
- Job DescriptionsDokument139 SeitenJob DescriptionsAbdullah Bin SaeedNoch keine Bewertungen
- Seminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathDokument18 SeitenSeminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathcastillojessNoch keine Bewertungen
- An Unconscious Patient With A DNR TattooDokument2 SeitenAn Unconscious Patient With A DNR TattoonadaNoch keine Bewertungen
- TORCHDokument32 SeitenTORCHJafar NoryNoch keine Bewertungen
- Medicina Chinesa JeremyDokument2 SeitenMedicina Chinesa JeremyJuan Gabriel CunhaNoch keine Bewertungen
- Acadia PharmaceuticalsDokument3 SeitenAcadia PharmaceuticalsAman DecoraterNoch keine Bewertungen
- Ashiq Tutorials 2008Dokument23 SeitenAshiq Tutorials 2008Sk ChaudhryNoch keine Bewertungen
- Annotated BibliographyDokument4 SeitenAnnotated BibliographyJuanNoch keine Bewertungen
- HSBDokument4 SeitenHSBCarlos WebsterNoch keine Bewertungen
- Lesson Plan On Spina BifidaDokument24 SeitenLesson Plan On Spina BifidaPriyaNoch keine Bewertungen
- Detoxification:Management of AmaDokument3 SeitenDetoxification:Management of AmaqueencelNoch keine Bewertungen