Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- 433 Psychiatry Team Child PsychiatryDokument10 Seiten433 Psychiatry Team Child PsychiatrySherlina Rintik Tirta AyuNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Avery Hayden - How To Attract WomenDokument143 SeitenAvery Hayden - How To Attract WomenAng3l Ang3l100% (1)
- Superficial Dermal Fillers With Hyaluronic AcidDokument5 SeitenSuperficial Dermal Fillers With Hyaluronic AcidchipanzeNoch keine Bewertungen
- The Procedure: Cleaning ValidationDokument4 SeitenThe Procedure: Cleaning ValidationYousif100% (1)
- PMS SopDokument8 SeitenPMS Sopstevekent40% (5)
- Gautam Das Clinical ExaminationDokument233 SeitenGautam Das Clinical ExaminationHenry SugihartoNoch keine Bewertungen
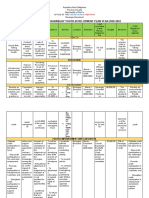
- Comprehensive Barangay Youth Development Plan Year 2020-2022Dokument7 SeitenComprehensive Barangay Youth Development Plan Year 2020-2022ralf100% (1)
- Ba - LLB (Hons.) Semester-1 Sociology Topic-Child Marriage-Factors, Problems and PreventionDokument20 SeitenBa - LLB (Hons.) Semester-1 Sociology Topic-Child Marriage-Factors, Problems and PreventionAkshat MishraNoch keine Bewertungen
- Physical Education and Health 12 - Q2 WEEK 7 8Dokument10 SeitenPhysical Education and Health 12 - Q2 WEEK 7 8Cristina Luz Cabana75% (4)
- Predicting Teenage Girls' Sexual Activity and Contraception Use: An Application of Matching LawDokument16 SeitenPredicting Teenage Girls' Sexual Activity and Contraception Use: An Application of Matching LawPedro Pablo OchoaNoch keine Bewertungen
- Lecture 5 Research Design Observational Studies (Descriptive and Cross Sectional) - Dr. Dr. Osman Sianipar, DMM., MSC., Sp. PK (K) (2022)Dokument49 SeitenLecture 5 Research Design Observational Studies (Descriptive and Cross Sectional) - Dr. Dr. Osman Sianipar, DMM., MSC., Sp. PK (K) (2022)Sheila Tirta AyumurtiNoch keine Bewertungen
- Northern India Textile Research Association, Ghaziabad: Antimicrobial (Anti Bacterial & Antifungal) TestingDokument2 SeitenNorthern India Textile Research Association, Ghaziabad: Antimicrobial (Anti Bacterial & Antifungal) TestingNitraNtcNoch keine Bewertungen
- CHN 1 - NCM 104 - RLE - Unit 3 - ContentDokument4 SeitenCHN 1 - NCM 104 - RLE - Unit 3 - ContentZahraJaneANoch keine Bewertungen
- HS7008 Module Guide T2 - 2019-20Dokument14 SeitenHS7008 Module Guide T2 - 2019-20OsamaMazhariNoch keine Bewertungen
- CHAPTER - 1 - Differential Diagnoses - 2011 - Small Animal Dermatology PDFDokument21 SeitenCHAPTER - 1 - Differential Diagnoses - 2011 - Small Animal Dermatology PDFRanjani RajasekaranNoch keine Bewertungen
- Nat BoardDokument93 SeitenNat BoardChintan C. Nishar100% (1)
- Midterm Exams NCM1531L - Care of The Older Persons LectureDokument50 SeitenMidterm Exams NCM1531L - Care of The Older Persons Lecturejjmaxh20Noch keine Bewertungen
- LEUKOcyte Counting LabDokument13 SeitenLEUKOcyte Counting Labsyed nomanshahNoch keine Bewertungen
- 1.2. PTI Insurance Benefits - English VersionDokument23 Seiten1.2. PTI Insurance Benefits - English VersionĐào Duy PhiNoch keine Bewertungen
- Biomolecules Practice AnswersDokument3 SeitenBiomolecules Practice AnswersNoura RoseNoch keine Bewertungen
- NOV. 2 - 6@ENGLISH 9 Learner Activity Sheet (LAS)Dokument4 SeitenNOV. 2 - 6@ENGLISH 9 Learner Activity Sheet (LAS)Maria BuizonNoch keine Bewertungen
- Computer-Assisted Osteotomy Guides and Pre-Bent Titanium Plates Improve The Planning For Correction of Facial AsymmetryDokument34 SeitenComputer-Assisted Osteotomy Guides and Pre-Bent Titanium Plates Improve The Planning For Correction of Facial AsymmetrySantos TicaNoch keine Bewertungen
- Manual 45001-2018Dokument34 SeitenManual 45001-2018Mohamed HabibNoch keine Bewertungen
- Ate Gabs Nyo Pagod NaDokument3 SeitenAte Gabs Nyo Pagod NaGabrielle EvangelistaNoch keine Bewertungen
- Course Learning Packets Template Saint Louis University School of Teacher Education and Liberal ArtsDokument8 SeitenCourse Learning Packets Template Saint Louis University School of Teacher Education and Liberal ArtsUchayyaNoch keine Bewertungen
- 1 Fundamentals of HRM1Dokument23 Seiten1 Fundamentals of HRM1Wael ALyNoch keine Bewertungen
- Efektivitas Aromaterapi Lemon Untuk Mengatasi Emesis GravidarumDokument8 SeitenEfektivitas Aromaterapi Lemon Untuk Mengatasi Emesis Gravidarumsri yulinar pakuNoch keine Bewertungen
- 2018 03 148 ManzellaDokument9 Seiten2018 03 148 ManzellaAomChanumpornNoch keine Bewertungen
- Eng 32 300Dokument269 SeitenEng 32 300DICKY WAHYUDI SIMBOLONNoch keine Bewertungen
- Microbiology of Concentrated MilkDokument30 SeitenMicrobiology of Concentrated MilkNitric AcidNoch keine Bewertungen