Das könnte Ihnen auch gefallen
- Orthok Case Reviews in Ophthalmology 2eDokument2 SeitenOrthok Case Reviews in Ophthalmology 2eDanielle SangalangNoch keine Bewertungen
- Advanced Slit Lamp Skills: How To Adjust The Lighting To See Stuff!Dokument45 SeitenAdvanced Slit Lamp Skills: How To Adjust The Lighting To See Stuff!Danielle SangalangNoch keine Bewertungen
- Conclusions Background: Vision Development & RehabilitationDokument13 SeitenConclusions Background: Vision Development & RehabilitationDanielle SangalangNoch keine Bewertungen
- Volume 6, Issue 1 - 1Dokument10 SeitenVolume 6, Issue 1 - 1Danielle SangalangNoch keine Bewertungen
- Myopic Changes in A Climber After Taking Acetazolamide and The Use of Corrective Lenses To Temporize Symptoms: A Case Report From Mount KilimanjaroDokument4 SeitenMyopic Changes in A Climber After Taking Acetazolamide and The Use of Corrective Lenses To Temporize Symptoms: A Case Report From Mount KilimanjaroDanielle SangalangNoch keine Bewertungen
- Corneal Injury Leads To Discovery: A Case Study On Asymptomatic AmblyopiaDokument1 SeiteCorneal Injury Leads To Discovery: A Case Study On Asymptomatic AmblyopiaDanielle SangalangNoch keine Bewertungen
- A Course in Low Vision Practice: P 5 - Magnification and MagnifiersDokument6 SeitenA Course in Low Vision Practice: P 5 - Magnification and MagnifiersDanielle SangalangNoch keine Bewertungen
- Alternating Horner Syndrome: Case Report and Review of The LiteratureDokument4 SeitenAlternating Horner Syndrome: Case Report and Review of The LiteratureDanielle SangalangNoch keine Bewertungen
- Clinical Characteristics of Exodeviated Patients With Accomodative Esotropia and Hyperopia Without StrabismusDokument5 SeitenClinical Characteristics of Exodeviated Patients With Accomodative Esotropia and Hyperopia Without StrabismusDanielle SangalangNoch keine Bewertungen
- Horner's Syndrome After Carotid Artery Stenting:: Case ReportDokument5 SeitenHorner's Syndrome After Carotid Artery Stenting:: Case ReportDanielle SangalangNoch keine Bewertungen
- Horners Syndrome Resulting From Agenesis of The Internal Carotid Artery: Report of A Third CaseDokument2 SeitenHorners Syndrome Resulting From Agenesis of The Internal Carotid Artery: Report of A Third CaseDanielle SangalangNoch keine Bewertungen
- Opht PDFDokument99 SeitenOpht PDFDanielle SangalangNoch keine Bewertungen
- Horner's Syndrome Due To A Large Schwannoma of The Cervical Sympathetic Chain: Report of CaseDokument4 SeitenHorner's Syndrome Due To A Large Schwannoma of The Cervical Sympathetic Chain: Report of CaseDanielle SangalangNoch keine Bewertungen
- Acquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDokument10 SeitenAcquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDanielle SangalangNoch keine Bewertungen
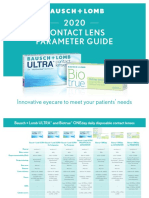
- 2020 Contact Lens Parameter Guide: Innovative Eyecare To Meet Your Patients' NeedsDokument4 Seiten2020 Contact Lens Parameter Guide: Innovative Eyecare To Meet Your Patients' NeedsDanielle SangalangNoch keine Bewertungen
- Horner's Syndrome During Spindle Cell Lipoma of The Neck - A CaseDokument4 SeitenHorner's Syndrome During Spindle Cell Lipoma of The Neck - A CaseDanielle SangalangNoch keine Bewertungen
- Horner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDokument3 SeitenHorner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDanielle SangalangNoch keine Bewertungen
- 09 OpticsDokument10 Seiten09 OpticsRena AdachiNoch keine Bewertungen
- The Other Amsler ChartsFINALDokument20 SeitenThe Other Amsler ChartsFINALDanielle SangalangNoch keine Bewertungen
- RPG Series Ophthalmology Buster PDFDokument299 SeitenRPG Series Ophthalmology Buster PDFDanielle SangalangNoch keine Bewertungen
- A Review of Ocular Genetics and Inherited Eye Diseases: SD MathebulaDokument12 SeitenA Review of Ocular Genetics and Inherited Eye Diseases: SD Mathebulalavinia diaNoch keine Bewertungen
- Clinical Optometry Primary Eye CareDokument3 SeitenClinical Optometry Primary Eye CareDanielle SangalangNoch keine Bewertungen
- Bino - Lec - Midterm Exam - Yellow - PadDokument11 SeitenBino - Lec - Midterm Exam - Yellow - PadDanielle SangalangNoch keine Bewertungen
- Geometrical and Visual OpticsDokument382 SeitenGeometrical and Visual OpticsWaleedAhmad100% (5)
- Clinical Orthoptics - Fiona Rowe - 146Dokument6 SeitenClinical Orthoptics - Fiona Rowe - 146Danielle SangalangNoch keine Bewertungen
- Infant ReflexesDokument14 SeitenInfant ReflexesJohn Agana AyamgaNoch keine Bewertungen
- Best Aid To Ophthalmology - Pramod TK - 318Dokument3 SeitenBest Aid To Ophthalmology - Pramod TK - 318Danielle SangalangNoch keine Bewertungen
- Clinical Procedures in Primary Eye Care-David Elliott - 158Dokument3 SeitenClinical Procedures in Primary Eye Care-David Elliott - 158Danielle SangalangNoch keine Bewertungen
- Binocular Vision & Orthoptics - Bruce Evans - 17Dokument3 SeitenBinocular Vision & Orthoptics - Bruce Evans - 17Danielle SangalangNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Sample Army Risk Assessment FormDokument3 SeitenSample Army Risk Assessment Formtachiwa100Noch keine Bewertungen
- Sprain Ankle JurnalDokument9 SeitenSprain Ankle JurnalRahmadanii RahmadaniiNoch keine Bewertungen
- Screenshot 2023-07-22 at 21.06.12Dokument28 SeitenScreenshot 2023-07-22 at 21.06.12ariNoch keine Bewertungen
- Lennox-VRF EHB VRF Three-PhaseDokument187 SeitenLennox-VRF EHB VRF Three-PhaseLouie Derek OrtizNoch keine Bewertungen
- Rangkuman Salter Bab 14Dokument64 SeitenRangkuman Salter Bab 14Febee NathaliaNoch keine Bewertungen
- Frida Kahlo PowerpointDokument30 SeitenFrida Kahlo Powerpointapi-335933103Noch keine Bewertungen
- Risk Assessment For Installation of Diesel Generator111111Dokument8 SeitenRisk Assessment For Installation of Diesel Generator111111Baher Mohamed100% (1)
- Rumah Sakit Mata ICD X Eng FixDokument11 SeitenRumah Sakit Mata ICD X Eng FixPelayanan MedisNoch keine Bewertungen
- Tugas English Nursing Prillisia DeazriDokument4 SeitenTugas English Nursing Prillisia DeazriPrillisia DeazriNoch keine Bewertungen
- 01 - BGMG CCT Education - Handout - Domestic Violence - 2021-06Dokument6 Seiten01 - BGMG CCT Education - Handout - Domestic Violence - 2021-06hopeand26Noch keine Bewertungen
- Q.P. Code: 278151: Answer ALL QuestionsDokument18 SeitenQ.P. Code: 278151: Answer ALL QuestionsR HariNoch keine Bewertungen
- Commoner - Bounty HunterDokument1 SeiteCommoner - Bounty HunterItzhakEvenNoch keine Bewertungen
- Unit 4: Medical EmergenciesDokument44 SeitenUnit 4: Medical EmergenciesMR々๛ AKMツNoch keine Bewertungen
- NEET PG 2015 Question Paper With SolutionsDokument1.852 SeitenNEET PG 2015 Question Paper With SolutionsSK RaulNoch keine Bewertungen
- Factors Affecting SafetyDokument31 SeitenFactors Affecting Safetyrahtu suzi ameliaNoch keine Bewertungen
- Talar Cyst: JSM Foot and AnkleDokument2 SeitenTalar Cyst: JSM Foot and Anklenpr00Noch keine Bewertungen
- SFSFSFDokument6 SeitenSFSFSFFatima MartinezNoch keine Bewertungen
- Assesment Competency ICD 10 For CodersDokument31 SeitenAssesment Competency ICD 10 For CodersDony Kristian100% (2)
- Ear Pain in Children Up To DateDokument25 SeitenEar Pain in Children Up To DateNicole Marie NicolasNoch keine Bewertungen
- عرض تقديمي 28Dokument33 Seitenعرض تقديمي 28saifmajidhammadiNoch keine Bewertungen
- Name of The Job Site: WIPRO IT SEZ Project, Kodathi, Bangalore Activity: MS, PVC Conduiting&Circuitwiring, Point WiringDokument8 SeitenName of The Job Site: WIPRO IT SEZ Project, Kodathi, Bangalore Activity: MS, PVC Conduiting&Circuitwiring, Point Wiringchaitanya snNoch keine Bewertungen
- Closed Legal MemoDokument8 SeitenClosed Legal Memogaming accountNoch keine Bewertungen
- Childhood Injuries and PoisoningDokument51 SeitenChildhood Injuries and PoisoningPatNoch keine Bewertungen
- RTPC101 Body System RootsDokument40 SeitenRTPC101 Body System RootsJazther CapiliNoch keine Bewertungen
- Hope 3 Module 6 Quarter 2Dokument16 SeitenHope 3 Module 6 Quarter 2Marchan Dalapo-Llacuna CorowanNoch keine Bewertungen
- Acute Subdural Hematoma Morbidity, Mortality and Operative TimingDokument7 SeitenAcute Subdural Hematoma Morbidity, Mortality and Operative TimingNadia BordaşNoch keine Bewertungen
- .... Anthelio Icd-10 Expresslearn: AmputationsDokument4 Seiten.... Anthelio Icd-10 Expresslearn: AmputationsAnne Rozette OngNoch keine Bewertungen
- Nerve Supply To The Upper Limb: Laura Jayne Watson November 13, 2015Dokument15 SeitenNerve Supply To The Upper Limb: Laura Jayne Watson November 13, 2015Hacker 75Noch keine Bewertungen
- Matrix MidfaceDokument24 SeitenMatrix MidfaceUNoch keine Bewertungen
- Exam CDI 313Dokument4 SeitenExam CDI 313Arianne FarnazoNoch keine Bewertungen