Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Electrolyte ImbalancesDokument4 SeitenElectrolyte ImbalancesMoni Mbumba MelekeNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Stomach and Duodenal UlcersDokument5 SeitenStomach and Duodenal UlcersYaniNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Vats Vs Chest Tube in Empysema in ChildrenDokument9 SeitenVats Vs Chest Tube in Empysema in ChildrenYaniNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Respiratory System DisorderDokument46 SeitenRespiratory System DisorderYaniNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
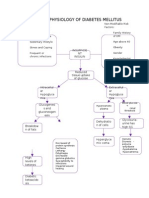
- Pathophysiology of Diabetes MellitusDokument8 SeitenPathophysiology of Diabetes MellitusYaniNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Abdominal PainDokument3 SeitenAbdominal PainYaniNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Thoracic TraumaDokument39 SeitenThoracic TraumaYaniNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Stomach and Duodenal UlcersDokument5 SeitenStomach and Duodenal UlcersYaniNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- All About ECGDokument151 SeitenAll About ECGSherwan R Shal94% (16)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Hematologic Problems LectureDokument87 SeitenHematologic Problems LectureYaniNoch keine Bewertungen
- Case On PnuemoniaDokument16 SeitenCase On PnuemoniaYaniNoch keine Bewertungen
- Dengue CaseDokument24 SeitenDengue CaseYaniNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Fluids and ElectrolytesDokument7 SeitenFluids and ElectrolytesAngelica QuimnoNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Benefits of Family Planning in The PhilippinesDokument6 SeitenBenefits of Family Planning in The PhilippinesYaniNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Tufts Opencourseware Case of EncephalitisDokument16 SeitenTufts Opencourseware Case of EncephalitisYaniNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Areas of SociologyDokument2 SeitenAreas of SociologyYaniNoch keine Bewertungen
- The World's Funniest ProverbsDokument160 SeitenThe World's Funniest Proverbsganapsin100% (2)
- Physiology of Diabetes MellitusDokument1 SeitePhysiology of Diabetes MellitusYaniNoch keine Bewertungen
- Hemmoragic Dengue FeverDokument2 SeitenHemmoragic Dengue FeverYaniNoch keine Bewertungen
- Loss Weight Forever - 50 Habits of Naturally Thin PeopleDokument8 SeitenLoss Weight Forever - 50 Habits of Naturally Thin PeopleSedeenaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Promotion Sexual Health OPAS OMS PDFDokument64 SeitenPromotion Sexual Health OPAS OMS PDFHerbert RodriguesNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Comprehensive Geriatric AssessmentDokument75 SeitenComprehensive Geriatric AssessmentBodat BodatsNoch keine Bewertungen
- RupatadineDokument1 SeiteRupatadinePiscean YangNoch keine Bewertungen
- Triage and assessment of multiple trauma patientsDokument5 SeitenTriage and assessment of multiple trauma patientsChristabel EdithNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Vit DDokument36 SeitenVit DConstantin MarioaraNoch keine Bewertungen
- PROMETRIC- NURSE SPECIALIST DIAGNOSTIC EXAMDokument9 SeitenPROMETRIC- NURSE SPECIALIST DIAGNOSTIC EXAMAyuy Welliss MedusaNoch keine Bewertungen
- Herpes Zoster OticusDokument12 SeitenHerpes Zoster Oticusraghad.bassalNoch keine Bewertungen
- Malabsorption Syndrome: Dr. Gehan Mohamed Dr. Abdelaty ShawkyDokument25 SeitenMalabsorption Syndrome: Dr. Gehan Mohamed Dr. Abdelaty ShawkyNikhil GuptaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Patient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalDokument5 SeitenPatient Information From Your Surgeon & Sages Laparoscopic Gallbladder RemovalolarrozaNoch keine Bewertungen
- International Travelers Medical Center PrescriptionDokument1 SeiteInternational Travelers Medical Center PrescriptionDeo Warren SilangNoch keine Bewertungen
- Upper Airway ObstructionDokument17 SeitenUpper Airway ObstructionRai Hana100% (1)
- Gallstones: Causes, Complications and Treatment OptionsDokument6 SeitenGallstones: Causes, Complications and Treatment Optionsricky aditNoch keine Bewertungen
- Preeclampsia With HELLP SyndromeDokument8 SeitenPreeclampsia With HELLP SyndromeWely Tiffani YpNoch keine Bewertungen
- Notes For NCM 109Dokument13 SeitenNotes For NCM 109Mae Arra Lecobu-anNoch keine Bewertungen
- 2010 Guideline AFDokument61 Seiten2010 Guideline AFyamtotlNoch keine Bewertungen
- Learning Objective Content Teaching Strategy Time Alloted EvaluationDokument3 SeitenLearning Objective Content Teaching Strategy Time Alloted EvaluationAmera DimatingcalNoch keine Bewertungen
- Guideline For Antimicrobial Use in The Orthopaedic and Trauma Department..Dokument8 SeitenGuideline For Antimicrobial Use in The Orthopaedic and Trauma Department..Long Nguyễn HoàngNoch keine Bewertungen
- PART I: Vocabulary (20 Items - 4,0 Pts - 0,2 PTS/ Item) Questions 1-5Dokument5 SeitenPART I: Vocabulary (20 Items - 4,0 Pts - 0,2 PTS/ Item) Questions 1-5Nguyễn TavirelNoch keine Bewertungen
- Peppermint Oil as an Effective Mosquito RepellentDokument4 SeitenPeppermint Oil as an Effective Mosquito RepellentKester PlaydaNoch keine Bewertungen
- Transfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDokument3 SeitenTransfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDR. KHANNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Abdominal Aortic Aneurysm Vascular SurgeryDokument2 SeitenAbdominal Aortic Aneurysm Vascular SurgeryzipzipzipNoch keine Bewertungen
- Microbial Food CantaminationDokument39 SeitenMicrobial Food CantaminationPrashant ItankarNoch keine Bewertungen
- RESEARCH 1 Fi 2Dokument20 SeitenRESEARCH 1 Fi 2Alondra SagarioNoch keine Bewertungen
- CV SAMEEP - PathologistDokument7 SeitenCV SAMEEP - PathologistMumtaj AnsariNoch keine Bewertungen
- Neurogenic Disorders of The LarynxDokument37 SeitenNeurogenic Disorders of The LarynxSyaffira SalsabilaNoch keine Bewertungen
- Protozoan Parasites: Infective Stages, Transmission, DiseasesDokument3 SeitenProtozoan Parasites: Infective Stages, Transmission, DiseasesPatrice Bianca SarmientoNoch keine Bewertungen
- Blood TransfusionDokument30 SeitenBlood TransfusionnoorgianilestariNoch keine Bewertungen
- The Complete Weight Loss Guide: Brought To You byDokument6 SeitenThe Complete Weight Loss Guide: Brought To You bySam YoussefNoch keine Bewertungen
- Drug Study FluvoxamineDokument2 SeitenDrug Study FluvoxamineAngeline de Gala0% (1)
- Important Instructions:: RadiotherapyDokument1 SeiteImportant Instructions:: RadiotherapySuranjan MaitraNoch keine Bewertungen
- Group 5 Research Paper 22the Causes of The Increasing Anxiety Amongst The Grade 10 Student of Maligaya Highschool22 1Dokument3 SeitenGroup 5 Research Paper 22the Causes of The Increasing Anxiety Amongst The Grade 10 Student of Maligaya Highschool22 1Lean De MesaNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)