Das könnte Ihnen auch gefallen
- Laborator DPDokument15 SeitenLaborator DPGabriela BaltatescuNoch keine Bewertungen
- EU Digital Pathology Workflow Guidelines 2021Dokument21 SeitenEU Digital Pathology Workflow Guidelines 2021patolog32Noch keine Bewertungen
- Digital Cytopathology JCDokument26 SeitenDigital Cytopathology JCAchin KumarNoch keine Bewertungen
- Campen EllaDokument21 SeitenCampen EllaWhy BotherNoch keine Bewertungen
- TLCR 09 05 2255Dokument22 SeitenTLCR 09 05 2255Vaishnavah SookrajhNoch keine Bewertungen
- Journal Pone 0269323Dokument13 SeitenJournal Pone 0269323sowmiNoch keine Bewertungen
- Comparative Analysis of Deep Learning Convolutional Neural Networks Based On Transfer Learning For Pneumonia DetectionDokument12 SeitenComparative Analysis of Deep Learning Convolutional Neural Networks Based On Transfer Learning For Pneumonia DetectionIJRASETPublicationsNoch keine Bewertungen
- Deep Convolutional Neural Networks in Thyroid Disease Detection-Full TextDokument10 SeitenDeep Convolutional Neural Networks in Thyroid Disease Detection-Full TextJamesLeeNoch keine Bewertungen
- Expert Systems With Applications: Tarig Faisal, Mohd Nasir Taib, Fatimah IbrahimDokument13 SeitenExpert Systems With Applications: Tarig Faisal, Mohd Nasir Taib, Fatimah IbrahimDwi Rahma YunikaNoch keine Bewertungen
- Pilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeDokument6 SeitenPilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeJoel TroyaNoch keine Bewertungen
- AI (Artificial Intelligence) in Histopathology - From Image Analysis To Automated DiagnosisDokument7 SeitenAI (Artificial Intelligence) in Histopathology - From Image Analysis To Automated DiagnosisMugundhan RamamoorthyNoch keine Bewertungen
- 1 s2.0 S1746809423012648 MainDokument18 Seiten1 s2.0 S1746809423012648 Mainmozhganeutoop1998Noch keine Bewertungen
- 1 s2.0 S1059131120303162 MainDokument9 Seiten1 s2.0 S1059131120303162 MainInes Arias PazNoch keine Bewertungen
- Ultrasound Imaging ThesisDokument7 SeitenUltrasound Imaging Thesisbrendazerrindependence100% (2)
- Covid19 and Pneumonia Detection Using Deep-LeaningDokument17 SeitenCovid19 and Pneumonia Detection Using Deep-LeaningIJRASETPublicationsNoch keine Bewertungen
- World'S First Known Open-Source Machine Learning Convolutional Artificial Neural Network in Covid19 Xray Diagnosis (February 9 2020)Dokument18 SeitenWorld'S First Known Open-Source Machine Learning Convolutional Artificial Neural Network in Covid19 Xray Diagnosis (February 9 2020)Shili WalaNoch keine Bewertungen
- Sensors 22 08497Dokument10 SeitenSensors 22 08497skgs1970Noch keine Bewertungen
- Pneumonia and COVID-19 Detection Using Convolutional Neural NetworkDokument10 SeitenPneumonia and COVID-19 Detection Using Convolutional Neural NetworkIJRASETPublicationsNoch keine Bewertungen
- Final Revision of Octane Paper For Nature MedicineDokument41 SeitenFinal Revision of Octane Paper For Nature MedicineElias Alboadicto Villagrán DonaireNoch keine Bewertungen
- Experimental Disease Prediction Research On Combining Natural Language Processing and Machine LearningDokument6 SeitenExperimental Disease Prediction Research On Combining Natural Language Processing and Machine Learningharshareddy96001Noch keine Bewertungen
- COVID Detection Using Symptoms and X-RayDokument10 SeitenCOVID Detection Using Symptoms and X-RayIJRASETPublicationsNoch keine Bewertungen
- Oncology Nursing Trends and Issues 3Dokument7 SeitenOncology Nursing Trends and Issues 3DaichiNoch keine Bewertungen
- Deep Learning For Classification and Localization of COVID-19 Markers in Point-Of-Care Lung UltrasoundDokument11 SeitenDeep Learning For Classification and Localization of COVID-19 Markers in Point-Of-Care Lung UltrasoundJohn NewcolasNoch keine Bewertungen
- Integration of Information Technologies in Clinical Studies in NicaraguaDokument6 SeitenIntegration of Information Technologies in Clinical Studies in NicaraguaIrien S HermanNoch keine Bewertungen
- Srep 12215Dokument8 SeitenSrep 12215endang linawati, drNoch keine Bewertungen
- Design: An Intelligent Multimedia Patients Information Problems and SolutionsDokument10 SeitenDesign: An Intelligent Multimedia Patients Information Problems and SolutionsFauzan KurniawanNoch keine Bewertungen
- Research Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationDokument9 SeitenResearch Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationNaoual NassiriNoch keine Bewertungen
- Disease Prediction Using Machine Learning Algorithms KNN and CNNDokument7 SeitenDisease Prediction Using Machine Learning Algorithms KNN and CNNIJRASETPublications100% (1)
- Applied Sciences: Smart HealthcareDokument5 SeitenApplied Sciences: Smart HealthcareSumathi GowdaNoch keine Bewertungen
- 1 s2.0 S2667099222000172 MainDokument14 Seiten1 s2.0 S2667099222000172 Mainadam wilsonNoch keine Bewertungen
- Digital Pathology and Artificial Intelligence As The Next Chapter in Diagnostic HematopathologyDokument7 SeitenDigital Pathology and Artificial Intelligence As The Next Chapter in Diagnostic HematopathologyKira Cao0% (1)
- Jimaging 07 00111Dokument19 SeitenJimaging 07 00111okuwobiNoch keine Bewertungen
- Deep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule IdentificationDokument9 SeitenDeep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule Identificationdreadrebirth2342Noch keine Bewertungen
- Running Title: Digital Vs Conventional Implant Impressions: DDS, MS, PHDDokument41 SeitenRunning Title: Digital Vs Conventional Implant Impressions: DDS, MS, PHDÁł ÃăNoch keine Bewertungen
- Cyt 34 5Dokument10 SeitenCyt 34 5Archondakis StavrosNoch keine Bewertungen
- Comparative Health Technology Assessment of Robotic-AssistedDokument9 SeitenComparative Health Technology Assessment of Robotic-AssistedDanica SavićNoch keine Bewertungen
- Barriers and Facilitators To Adoption of Soft Copy Interpretation From The User PerspectiveDokument9 SeitenBarriers and Facilitators To Adoption of Soft Copy Interpretation From The User PerspectiveIT LicensingNoch keine Bewertungen
- Disease Prediction Using Machine LearningDokument9 SeitenDisease Prediction Using Machine LearningIJRASETPublicationsNoch keine Bewertungen
- Tema 10 TelepracticaaudiologicaDokument8 SeitenTema 10 TelepracticaaudiologicaManecita CoqNoch keine Bewertungen
- Artificial Intelligence For Blood AnalysisDokument14 SeitenArtificial Intelligence For Blood AnalysisKIPNGENO EMMANUELNoch keine Bewertungen
- Prediction of Pneumonia Using CNNDokument9 SeitenPrediction of Pneumonia Using CNNIJRASETPublicationsNoch keine Bewertungen
- Final ProjectDokument14 SeitenFinal Projectapi-298975236Noch keine Bewertungen
- Machine Learning Models Predicting Undertriage in Telephone TriageDokument9 SeitenMachine Learning Models Predicting Undertriage in Telephone TriageBudi RiyantoPrabowoNoch keine Bewertungen
- Transfer LearningDokument7 SeitenTransfer LearningAdah EneNoch keine Bewertungen
- Pulmonary Image Classification Based On Inception-V3 Transfer Learning ModelDokument9 SeitenPulmonary Image Classification Based On Inception-V3 Transfer Learning ModelKhaleda AkhterNoch keine Bewertungen
- A Neuro-Heuristic Approach For Recognition of Lung Diseases From X-RayDokument15 SeitenA Neuro-Heuristic Approach For Recognition of Lung Diseases From X-RaySarah NixonNoch keine Bewertungen
- 1 s2.0 S0957417422016372 MainDokument14 Seiten1 s2.0 S0957417422016372 MainMd NahiduzzamanNoch keine Bewertungen
- Vander Laak 2021Dokument10 SeitenVander Laak 2021typp3t5r3gzNoch keine Bewertungen
- Pneumonia Detection Using Convolutional Neural Networks (CNNS)Dokument14 SeitenPneumonia Detection Using Convolutional Neural Networks (CNNS)shekhar1405Noch keine Bewertungen
- Applied Sciences: A Novel Transfer Learning Based Approach For Pneumonia Detection in Chest X-Ray ImagesDokument17 SeitenApplied Sciences: A Novel Transfer Learning Based Approach For Pneumonia Detection in Chest X-Ray ImagesmzshaikhNoch keine Bewertungen
- RetrieveDokument13 SeitenRetrieveNEUMOLOGIA TLAHUACNoch keine Bewertungen
- Hybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesDokument14 SeitenHybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesMurshedul ArifeenNoch keine Bewertungen
- Realistic Simulation of Virtual Multi-Scale MultiDokument15 SeitenRealistic Simulation of Virtual Multi-Scale MultiSalma BouaziziNoch keine Bewertungen
- Radiation Exposure From CT in Early Childhood: A French Large-Scale Multicentre StudyDokument8 SeitenRadiation Exposure From CT in Early Childhood: A French Large-Scale Multicentre StudyArizal FuadNoch keine Bewertungen
- Multi-Channel Deep Convolutional Neural Networks For Multi-Classifying Thyroid DiseaseDokument14 SeitenMulti-Channel Deep Convolutional Neural Networks For Multi-Classifying Thyroid DiseaseRihab BEN LAMINENoch keine Bewertungen
- The Histopathological Diagnosis of Atypical Meningioma - Glass Slide Versus Whole Slide Imaging For Grading AssessmentDokument10 SeitenThe Histopathological Diagnosis of Atypical Meningioma - Glass Slide Versus Whole Slide Imaging For Grading AssessmentHastrina MailaniNoch keine Bewertungen
- (IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaDokument4 Seiten(IJCST-V11I3P1) :Dr.P.Bhaskar Naidu, P.Mary Harika, J.Pavani, B.Divyadhatri, J.ChandanaEighthSenseGroupNoch keine Bewertungen
- Covi-Assist Automatic COVID-19 Detection From Chest X-RaysDokument10 SeitenCovi-Assist Automatic COVID-19 Detection From Chest X-RaysIJRASETPublicationsNoch keine Bewertungen
- A Publicly Accessible Global Data Repository - The WHO TB-IPD PlatformDokument3 SeitenA Publicly Accessible Global Data Repository - The WHO TB-IPD Platformstephenpillar1718Noch keine Bewertungen
- Digital Radiography: Physical Principles and Quality ControlVon EverandDigital Radiography: Physical Principles and Quality ControlNoch keine Bewertungen
- A Multidisciplinary, Team-Based Teleconsultation Approach To Enhance Child Mental Health Services in Rural PediatricsDokument27 SeitenA Multidisciplinary, Team-Based Teleconsultation Approach To Enhance Child Mental Health Services in Rural PediatricslizetNoch keine Bewertungen
- Modeling The Spatial Distribution of Cancer and Determining The AssociatedDokument15 SeitenModeling The Spatial Distribution of Cancer and Determining The AssociatedlizetNoch keine Bewertungen
- Research On Teleconsultation Service Quality Based On Multi-Granularity Linguistic InformationDokument13 SeitenResearch On Teleconsultation Service Quality Based On Multi-Granularity Linguistic InformationlizetNoch keine Bewertungen
- Moura Et Al., 2018Dokument9 SeitenMoura Et Al., 2018Dayanne MonielleNoch keine Bewertungen
- Community Based Telepsychiatry Service For Older Adults Residing in A Rural and Remote Region-Utilization Pattern and Satisfaction Among StakeholdersDokument14 SeitenCommunity Based Telepsychiatry Service For Older Adults Residing in A Rural and Remote Region-Utilization Pattern and Satisfaction Among StakeholderslizetNoch keine Bewertungen
- 2.-Satisfaction With Rural Rheumatology Telemedicine ServiceDokument12 Seiten2.-Satisfaction With Rural Rheumatology Telemedicine ServicelizetNoch keine Bewertungen
- 1.-Teleconsultation For Clinicians Who Provide Human Immunodeficiency Virus CareDokument6 Seiten1.-Teleconsultation For Clinicians Who Provide Human Immunodeficiency Virus CarelizetNoch keine Bewertungen
- PHARMCARD Cardiology 2014Dokument294 SeitenPHARMCARD Cardiology 2014lizetNoch keine Bewertungen
- Biología MarinaDokument489 SeitenBiología MarinalizetNoch keine Bewertungen
- Supracrestal FiberotomyDokument6 SeitenSupracrestal FiberotomylizetNoch keine Bewertungen
- CURSO CRASH Lo Escencial en El Sistema NerviosoDokument282 SeitenCURSO CRASH Lo Escencial en El Sistema NerviosoEla Drzewiecka100% (1)
- Stability and RetentionDokument8 SeitenStability and RetentionlizetNoch keine Bewertungen
- Human Dimension & Interior Space (By Julius Panero and Martin Zelnik) - Ergonomia e AntropometriaDokument154 SeitenHuman Dimension & Interior Space (By Julius Panero and Martin Zelnik) - Ergonomia e AntropometriaTijana Gnjidić91% (157)
- Nociones de Derecho Civil y Mercantil 1 To 80Dokument80 SeitenNociones de Derecho Civil y Mercantil 1 To 80lizet100% (2)
- Biología MarinaDokument489 SeitenBiología MarinalizetNoch keine Bewertungen
- Main Relief Valve and Waste Cone - : Submittal DrawingDokument2 SeitenMain Relief Valve and Waste Cone - : Submittal Drawingumair186Noch keine Bewertungen
- Air BNB PaperDokument17 SeitenAir BNB Paperdummyrequester3Noch keine Bewertungen
- AC TEX250H - Spare Parts ListDokument9 SeitenAC TEX250H - Spare Parts ListValourdos LukasNoch keine Bewertungen
- The Inbound Sales Playbook - Interactive PDF by Articulate MarketingDokument23 SeitenThe Inbound Sales Playbook - Interactive PDF by Articulate MarketingSacha BismuthNoch keine Bewertungen
- TeklaDokument13 SeitenTeklaKamal MousserNoch keine Bewertungen
- #1 Business Plan For Small Business by SlidesgoDokument56 Seiten#1 Business Plan For Small Business by SlidesgoAdriana Osorio PalacinNoch keine Bewertungen
- Australian Standard: Engine Coolants Type A and Type B For Engine Cooling SystemsDokument7 SeitenAustralian Standard: Engine Coolants Type A and Type B For Engine Cooling Systemsocto widodoNoch keine Bewertungen
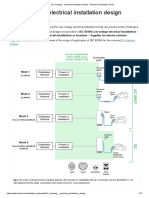
- EV Charging - Electrical Installation DesignDokument17 SeitenEV Charging - Electrical Installation Designetnanto100% (1)
- Allianz Cover LetterDokument4 SeitenAllianz Cover Letterc2z7wekb100% (1)
- IR ADV C7055 Series (SM)Dokument1.821 SeitenIR ADV C7055 Series (SM)Model MNoch keine Bewertungen
- Smart Prospecting That Works Every Time Krause en 19173Dokument6 SeitenSmart Prospecting That Works Every Time Krause en 19173rdeepak99Noch keine Bewertungen
- Proctored Mock Exam Guidelines 2021Dokument6 SeitenProctored Mock Exam Guidelines 2021Rahul SharmaNoch keine Bewertungen
- Capstone Project Report (AST)Dokument44 SeitenCapstone Project Report (AST)MSV ForeverNoch keine Bewertungen
- C18 OM Manual PDFDokument116 SeitenC18 OM Manual PDFMommy Mimma100% (3)
- Definition of Terms in REVITDokument33 SeitenDefinition of Terms in REVITMk GonzalesNoch keine Bewertungen
- Smartaisle Containment Brochure EnglishDokument32 SeitenSmartaisle Containment Brochure EnglishAsad NizamNoch keine Bewertungen
- Certificate of Good StandingDokument2 SeitenCertificate of Good StandingBhavesh MahajanNoch keine Bewertungen
- Site Acceptance/Change Form: Classification: Mobily INTERNAL USEDokument1 SeiteSite Acceptance/Change Form: Classification: Mobily INTERNAL USEqaisersiddiNoch keine Bewertungen
- Section IV Evaluation Criteria ITB16706Dokument3 SeitenSection IV Evaluation Criteria ITB16706IslamNoch keine Bewertungen
- For 21042021Dokument10 SeitenFor 21042021joydipindraniNoch keine Bewertungen
- Al-Amara 4 X 125Mw 9E: Spare Part List For Erection, Commissioning, and Start-UpDokument8 SeitenAl-Amara 4 X 125Mw 9E: Spare Part List For Erection, Commissioning, and Start-UpElias Abu FakherNoch keine Bewertungen
- IV B. TECH (Chemical Engineering) I SemesterDokument14 SeitenIV B. TECH (Chemical Engineering) I SemesterPiyush AmbulgekarNoch keine Bewertungen
- 5 - Network Flow ProblemsDokument30 Seiten5 - Network Flow ProblemsKaran KumarNoch keine Bewertungen
- Sudoku Using Constraint SatisfactionDokument12 SeitenSudoku Using Constraint SatisfactionTyler DerdunNoch keine Bewertungen
- Game Development With Unreal EngineDokument263 SeitenGame Development With Unreal EnginesrinivasappsdeveloperNoch keine Bewertungen
- GPK2 PN 500: 2-Way High Pressure Ball ValvesDokument4 SeitenGPK2 PN 500: 2-Way High Pressure Ball ValvesRolando Jara YoungNoch keine Bewertungen
- Learning DjangoDokument228 SeitenLearning DjangoSunil SinghNoch keine Bewertungen
- Srwa 3Dokument7 SeitenSrwa 3chaossang2Noch keine Bewertungen
- Ip210a Ip210Dokument3 SeitenIp210a Ip210Tudor SasuNoch keine Bewertungen
- Asdo Tie Bar Design Capacities: Product DataDokument2 SeitenAsdo Tie Bar Design Capacities: Product DatasivakumarNoch keine Bewertungen