Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Drug Study Guide Calculation PDFDokument49 SeitenDrug Study Guide Calculation PDFHarley Justiniani Dela CruzNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 2019 Focus Charting FDARDokument15 Seiten2019 Focus Charting FDARHarley Justiniani Dela Cruz25% (4)
- Decompression Sickness and Gas Embolism: Mohammad Guritno SURYOKUSUMODokument47 SeitenDecompression Sickness and Gas Embolism: Mohammad Guritno SURYOKUSUMOarinindyaNoch keine Bewertungen
- Pediatric Nursing ReviewDokument45 SeitenPediatric Nursing Reviewɹǝʍdןnos98% (87)
- UHMS HBO2 Indications 13th Ed. Front Matter ReferencesDokument172 SeitenUHMS HBO2 Indications 13th Ed. Front Matter ReferencesJeffry Hertanto50% (2)
- Anaesthetic Crisis ManualDokument63 SeitenAnaesthetic Crisis ManualkushishaNoch keine Bewertungen
- SP30 Neonatal Umbilical Vessel Catherization (Neonatal)Dokument13 SeitenSP30 Neonatal Umbilical Vessel Catherization (Neonatal)Ritzjerald Christer Abrena PahilanNoch keine Bewertungen
- Pulmonary EmbolismDokument23 SeitenPulmonary EmbolismBianca Dizon0% (1)
- Collecting Subjective and Objective Data 1.2.1Dokument9 SeitenCollecting Subjective and Objective Data 1.2.1Harley Justiniani Dela CruzNoch keine Bewertungen
- Anaesthesia For LapDokument91 SeitenAnaesthesia For LapAbhyuday KumarNoch keine Bewertungen
- Philippine Health Agenda - Dec1 - 1 PDFDokument26 SeitenPhilippine Health Agenda - Dec1 - 1 PDFreyalene gallegosNoch keine Bewertungen
- Head Eyes Ear Assessment 1Dokument20 SeitenHead Eyes Ear Assessment 1Harley Justiniani Dela CruzNoch keine Bewertungen
- APGAR-Scenario EXERCISESDokument1 SeiteAPGAR-Scenario EXERCISESHarley Justiniani Dela CruzNoch keine Bewertungen
- Apgar Score ChartDokument6 SeitenApgar Score ChartHarley Justiniani Dela CruzNoch keine Bewertungen
- APGAR-Scenario EXERCISESDokument1 SeiteAPGAR-Scenario EXERCISESHarley Justiniani Dela CruzNoch keine Bewertungen
- APGAR-Scenario EXERCISESDokument1 SeiteAPGAR-Scenario EXERCISESHarley Justiniani Dela CruzNoch keine Bewertungen
- IV Fluid ChartDokument2 SeitenIV Fluid Charthady920Noch keine Bewertungen
- 2020 Eric Erickson Psychoanalysis TheoryDokument29 Seiten2020 Eric Erickson Psychoanalysis TheoryHarley Justiniani Dela CruzNoch keine Bewertungen
- Assessment of The Skin, Hair and Nails I. Skin, Hair and NailsDokument12 SeitenAssessment of The Skin, Hair and Nails I. Skin, Hair and NailsHarley Justiniani Dela CruzNoch keine Bewertungen
- 2020 Physical Assessment of The ChildDokument11 Seiten2020 Physical Assessment of The ChildHarley Justiniani Dela CruzNoch keine Bewertungen
- Mac Peds FormularyDokument45 SeitenMac Peds FormularyLUIS MIGUEL CASTILLA MORANNoch keine Bewertungen
- 2021 Introduction To HealthDokument1 Seite2021 Introduction To HealthHarley Justiniani Dela CruzNoch keine Bewertungen
- MS Icu ErDokument2 SeitenMS Icu ErHarley Justiniani Dela CruzNoch keine Bewertungen
- MioticsDokument8 SeitenMioticsHarley Justiniani Dela CruzNoch keine Bewertungen
- IV Fluids - January 2019Dokument6 SeitenIV Fluids - January 2019Benjamin NgNoch keine Bewertungen
- 2020 Uhc-IrrDokument60 Seiten2020 Uhc-IrrHarley Justiniani Dela CruzNoch keine Bewertungen
- What Is A Cystoscopy?Dokument3 SeitenWhat Is A Cystoscopy?Harley Justiniani Dela Cruz100% (1)
- 2020 Bronchoscopy CaseDokument4 Seiten2020 Bronchoscopy CaseHarley Justiniani Dela CruzNoch keine Bewertungen
- 2020 IV Complications-Chapter27Dokument20 Seiten2020 IV Complications-Chapter27Harley Justiniani Dela CruzNoch keine Bewertungen
- 2020 Rle THFS Group AssignmentDokument1 Seite2020 Rle THFS Group AssignmentHarley Justiniani Dela CruzNoch keine Bewertungen
- 2019 Different Types of Doctor's OrderDokument1 Seite2019 Different Types of Doctor's OrderHarley Justiniani Dela CruzNoch keine Bewertungen
- Focus ChartingDokument3 SeitenFocus ChartingHarley Justiniani Dela CruzNoch keine Bewertungen
- 2017 Free Nursing Board Exam ReviewerDokument79 Seiten2017 Free Nursing Board Exam ReviewerHarley Justiniani Dela CruzNoch keine Bewertungen
- 2013 Quiz Bee QuestionsDokument2 Seiten2013 Quiz Bee QuestionsHarley Justiniani Dela CruzNoch keine Bewertungen
- 2017 Fluid and Electrolytes LECTURE NOTESDokument34 Seiten2017 Fluid and Electrolytes LECTURE NOTESHarley Justiniani Dela CruzNoch keine Bewertungen
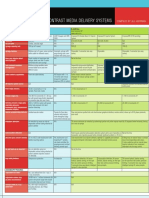
- Chart Smart Contrast Media Delivery SystemsDokument3 SeitenChart Smart Contrast Media Delivery SystemsaliNoch keine Bewertungen
- 2012 EO2 Student HB v1.0Dokument78 Seiten2012 EO2 Student HB v1.0Ariane HoffmannNoch keine Bewertungen
- 2013 - Contrast - Media - ACR v.9Dokument128 Seiten2013 - Contrast - Media - ACR v.9aegysabetterwayNoch keine Bewertungen
- In-Depth Review: Manish Saha and Michael AllonDokument13 SeitenIn-Depth Review: Manish Saha and Michael AllonKarthik SNoch keine Bewertungen
- Operating Table2Dokument11 SeitenOperating Table2Yhoyho Akhilun Dewa MimpiNoch keine Bewertungen
- Review Ct-GuidingDokument10 SeitenReview Ct-GuidingHeru SigitNoch keine Bewertungen
- Iosh Diving Presentation 001 Low Res Email Copy1Dokument49 SeitenIosh Diving Presentation 001 Low Res Email Copy1RajendraNoch keine Bewertungen
- CVP MonitoringDokument24 SeitenCVP MonitoringChoji Heiwajima100% (1)
- The Purpose of IV TherapyDokument5 SeitenThe Purpose of IV TherapyBilly Ray Villanueva100% (1)
- CVC RemovalDokument5 SeitenCVC RemovalRiza ZaharaNoch keine Bewertungen
- A Case of Decompression Illness Not Responding To Hyperbaric OxygenDokument4 SeitenA Case of Decompression Illness Not Responding To Hyperbaric OxygenYanny LabokNoch keine Bewertungen
- 2021 Hemodialysis Emergencies Core Curriculum 2021Dokument14 Seiten2021 Hemodialysis Emergencies Core Curriculum 2021Ale GutiérrezNoch keine Bewertungen
- Accidental Intravenous Infusion of Air: A Concise ReviewDokument5 SeitenAccidental Intravenous Infusion of Air: A Concise ReviewSiswand BIn Mohd AliNoch keine Bewertungen
- DHM 2017 - Mathieu - 10th ECHM Consensus Conference Recommendations On HBODokument9 SeitenDHM 2017 - Mathieu - 10th ECHM Consensus Conference Recommendations On HBODian Ayu SafitriNoch keine Bewertungen
- Mfa Ref Question BankDokument33 SeitenMfa Ref Question BankShivashish SharmaNoch keine Bewertungen
- Moon 2008Dokument37 SeitenMoon 2008Syafira NurfitriNoch keine Bewertungen
- 1 Environmental Physiology and Diving MedicineDokument10 Seiten1 Environmental Physiology and Diving MedicinededdyNoch keine Bewertungen
- Bard Magnum Manual de UsuarioDokument144 SeitenBard Magnum Manual de UsuarioNelson LebronNoch keine Bewertungen
- Sport Diving-CompletedDokument66 SeitenSport Diving-CompletedMuthu KumarNoch keine Bewertungen
- Prime The Line! A Case Report of Air Embolism From A Peripheral IV Line in The FieldDokument10 SeitenPrime The Line! A Case Report of Air Embolism From A Peripheral IV Line in The FieldLisete NunesNoch keine Bewertungen
- Concise Clinical Review: Diving MedicineDokument8 SeitenConcise Clinical Review: Diving MedicineJesús A Cárdenas RNoch keine Bewertungen
- Cooper Dan Brady, 2000Dokument20 SeitenCooper Dan Brady, 2000Jonathan LucisNoch keine Bewertungen
- Air Embolism - Practical Tips For Prevention and TreatmentDokument13 SeitenAir Embolism - Practical Tips For Prevention and TreatmentAdsoni IndoNoch keine Bewertungen
- Moot ProblemDokument20 SeitenMoot ProblemtaapqNoch keine Bewertungen