Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFDokument10 Seiten(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Cardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DDokument36 SeitenCardiology An Introduction: 12 Cardiomyopathy With Joseph S. Alpert, M.DpasambalyrradjohndarNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Application For Academic RecordDokument1 SeiteApplication For Academic RecordpasambalyrradjohndarNoch keine Bewertungen
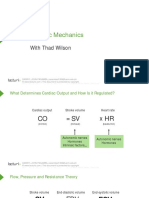
- Cardiac Mechanics: With Thad WilsonDokument26 SeitenCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Monthly Blood Glucose Diary PDFDokument1 SeiteMonthly Blood Glucose Diary PDFpasambalyrradjohndarNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Cardiac Cycle: With Thad WilsonDokument25 SeitenCardiac Cycle: With Thad WilsonpasambalyrradjohndarNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Loop Diuretics: Producers of The Greatest Diuresis With Rhonda LawesDokument23 SeitenLoop Diuretics: Producers of The Greatest Diuresis With Rhonda LawespasambalyrradjohndarNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Recording The Medical HistoryDokument8 SeitenRecording The Medical HistorypasambalyrradjohndarNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- (CLINPATH) 2.02 Transfusion II - Dr.-VillamayorDokument7 Seiten(CLINPATH) 2.02 Transfusion II - Dr.-VillamayorpasambalyrradjohndarNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Psych Osce Reviewer 1Dokument10 SeitenPsych Osce Reviewer 1pasambalyrradjohndarNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- 8 Part Eye Exam RevisedDokument17 Seiten8 Part Eye Exam RevisedpasambalyrradjohndarNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Psych Osce Reviewer 1Dokument10 SeitenPsych Osce Reviewer 1pasambalyrradjohndarNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- 8 Part Eye Exam RevisedDokument17 Seiten8 Part Eye Exam RevisedpasambalyrradjohndarNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmciDokument3 SeitenA Cross-Sectional Study On The Association Between Screen Time Exposure and Concentration Among Undergraduate University Students of UermmmcipasambalyrradjohndarNoch keine Bewertungen
- Charcoal Tracing Revised - ResultsDokument3 SeitenCharcoal Tracing Revised - ResultspasambalyrradjohndarNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Promissory NoteDokument1 SeitePromissory NotepasambalyrradjohndarNoch keine Bewertungen
- Oral Rehydration TherapyDokument12 SeitenOral Rehydration TherapypasambalyrradjohndarNoch keine Bewertungen
- Amoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebaDokument1 SeiteAmoeba: Cytoplasm (Both in Cyst and Peripheral Chromatin (Both Trophozoite Cyst AmoebapasambalyrradjohndarNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- PATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - YanezDokument8 SeitenPATHO 1.01a Cellular Response To Stress and Toxic Insults Part I - Yanezpasambalyrradjohndar100% (1)
- 3 Carbohydrates' StructureDokument33 Seiten3 Carbohydrates' StructureDilan TeodoroNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Corrosion Fatigue Phenomena Learned From Failure AnalysisDokument10 SeitenCorrosion Fatigue Phenomena Learned From Failure AnalysisDavid Jose Velandia MunozNoch keine Bewertungen
- Deal Report Feb 14 - Apr 14Dokument26 SeitenDeal Report Feb 14 - Apr 14BonviNoch keine Bewertungen
- ISBN Safe Work Method Statements 2022 03Dokument8 SeitenISBN Safe Work Method Statements 2022 03Tamo Kim ChowNoch keine Bewertungen
- Fss Presentation Slide GoDokument13 SeitenFss Presentation Slide GoReinoso GreiskaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Origami Oso HormigueroDokument9 SeitenOrigami Oso HormigueroRogelio CerdaNoch keine Bewertungen
- The Indonesia National Clean Development Mechanism Strategy StudyDokument223 SeitenThe Indonesia National Clean Development Mechanism Strategy StudyGedeBudiSuprayogaNoch keine Bewertungen
- Assembler Pass 2Dokument5 SeitenAssembler Pass 2AnuNoch keine Bewertungen
- ISO 9001 2015 AwarenessDokument23 SeitenISO 9001 2015 AwarenessSeni Oke0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Activity # 1 (DRRR)Dokument2 SeitenActivity # 1 (DRRR)Juliana Xyrelle FutalanNoch keine Bewertungen
- CAT 320D2: Hydraulic ExcavatorDokument5 SeitenCAT 320D2: Hydraulic Excavatorhydeer 13Noch keine Bewertungen
- De Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File NgheDokument10 SeitenDe Thi Hoc Ki 1 Mon Tieng Anh Lop 5 Co File Nghetuyen truongNoch keine Bewertungen
- Fusion Implementing Offerings Using Functional Setup Manager PDFDokument51 SeitenFusion Implementing Offerings Using Functional Setup Manager PDFSrinivasa Rao Asuru0% (1)
- Recommendations For Students With High Functioning AutismDokument7 SeitenRecommendations For Students With High Functioning AutismLucia SaizNoch keine Bewertungen
- Time-Sensitive Networking - An IntroductionDokument5 SeitenTime-Sensitive Networking - An Introductionsmyethdrath24Noch keine Bewertungen
- Financial Accounting 2 SummaryDokument10 SeitenFinancial Accounting 2 SummaryChoong Xin WeiNoch keine Bewertungen
- Functional DesignDokument17 SeitenFunctional DesignRajivSharmaNoch keine Bewertungen
- Sba 2Dokument29 SeitenSba 2api-377332228Noch keine Bewertungen
- Nama: Yossi Tiara Pratiwi Kelas: X Mis 1 Mata Pelajaran: Bahasa InggrisDokument2 SeitenNama: Yossi Tiara Pratiwi Kelas: X Mis 1 Mata Pelajaran: Bahasa InggrisOrionj jrNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Comparitive Study ICICI & HDFCDokument22 SeitenComparitive Study ICICI & HDFCshah faisal100% (1)
- Presentation 11Dokument14 SeitenPresentation 11stellabrown535Noch keine Bewertungen
- Law of EvidenceDokument14 SeitenLaw of EvidenceIsha ChavanNoch keine Bewertungen
- Prelim Examination MaternalDokument23 SeitenPrelim Examination MaternalAaron ConstantinoNoch keine Bewertungen
- Report On GDP of Top 6 Countries.: Submitted To: Prof. Sunil MadanDokument5 SeitenReport On GDP of Top 6 Countries.: Submitted To: Prof. Sunil MadanAbdullah JamalNoch keine Bewertungen
- Assignment#10 Global Strategy and The Multinational CorporationDokument1 SeiteAssignment#10 Global Strategy and The Multinational CorporationAnjaneth A. VillegasNoch keine Bewertungen
- Gemini Dollar WhitepaperDokument7 SeitenGemini Dollar WhitepaperdazeeeNoch keine Bewertungen
- Report Card Grade 1 2Dokument3 SeitenReport Card Grade 1 2Mely DelacruzNoch keine Bewertungen
- Lesson 5 Designing and Developing Social AdvocacyDokument27 SeitenLesson 5 Designing and Developing Social Advocacydaniel loberizNoch keine Bewertungen
- Dtu Placement BrouchureDokument25 SeitenDtu Placement BrouchureAbhishek KumarNoch keine Bewertungen
- 04 - Fetch Decode Execute Cycle PDFDokument3 Seiten04 - Fetch Decode Execute Cycle PDFShaun HaxaelNoch keine Bewertungen