Das könnte Ihnen auch gefallen
- Mastitis Prevention and TreatmentDokument25 SeitenMastitis Prevention and TreatmentGeetha SoundaryaNoch keine Bewertungen
- Simple Indigestion in RuminantsDokument11 SeitenSimple Indigestion in RuminantsAli H. Sadiek أ.د. علي حسن صديق75% (4)
- Gallstone DiseaseDokument14 SeitenGallstone DiseaseSuryaAtmajayaNoch keine Bewertungen
- Obstetrical Instruments and Their Use in Veterinary ObstetricsDokument3 SeitenObstetrical Instruments and Their Use in Veterinary Obstetricskrushna lamani100% (1)
- Lecture 9. Marketing and TransportDokument18 SeitenLecture 9. Marketing and TransportDr Jay bikram shahNoch keine Bewertungen
- 68 Abnormal PeuperiumDokument44 Seiten68 Abnormal PeuperiumGodsonYeboah-AwudziNoch keine Bewertungen
- 02 Fertilization & ImplantationDokument24 Seiten02 Fertilization & ImplantationAugust Ridlof RiwuNoch keine Bewertungen
- Rumen MotilityDokument32 SeitenRumen MotilityAbhay Singh100% (1)
- Psychological Perspective of Abnormal LaborDokument25 SeitenPsychological Perspective of Abnormal LaborPriscilla Sarah PayneNoch keine Bewertungen
- Pyometra& Endometritis in CattleDokument40 SeitenPyometra& Endometritis in CattleJibachha ShahNoch keine Bewertungen
- Physiology of GIT (2) (Autosaved)Dokument67 SeitenPhysiology of GIT (2) (Autosaved)RISALATUL KHOIROTUNISANoch keine Bewertungen
- Postpartum Uterine Infection in CattleDokument26 SeitenPostpartum Uterine Infection in CattleDilip GuptaNoch keine Bewertungen
- VVF Clinical Presentation 1Dokument24 SeitenVVF Clinical Presentation 1georgeloto12Noch keine Bewertungen
- Oxytocic & TocolyticDokument12 SeitenOxytocic & TocolyticFahmi Dwika Hafiz TrionoNoch keine Bewertungen
- Intussusception: Prepared By: Aisha H. AlaghaDokument20 SeitenIntussusception: Prepared By: Aisha H. AlaghaaiooshaNoch keine Bewertungen
- Hypertrophic Pyloric StenosisDokument23 SeitenHypertrophic Pyloric StenosisRahel Imelda PanggabeanNoch keine Bewertungen
- Care of HemophiliaDokument7 SeitenCare of HemophiliaBasant karn100% (4)
- Breast Pumps: PRESENTED BY: Shristi PanthaDokument16 SeitenBreast Pumps: PRESENTED BY: Shristi PanthaShristi PanthaNoch keine Bewertungen
- Operative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Dokument71 SeitenOperative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Jhon Negesse100% (1)
- Parturition Related Disorders in Sheep and Goat: G.N.PurohitDokument36 SeitenParturition Related Disorders in Sheep and Goat: G.N.PurohitgnpobsNoch keine Bewertungen
- Drugs and Dosages PDFDokument4 SeitenDrugs and Dosages PDFsharmee sarmientaNoch keine Bewertungen
- Liver: DR Kiran ShahidDokument21 SeitenLiver: DR Kiran ShahidYashfa Yasin100% (1)
- Active Management of Normal LabourDokument16 SeitenActive Management of Normal LabourjincyneeleshNoch keine Bewertungen
- Anorectal Malformations: Presented by Khushveer KaurDokument91 SeitenAnorectal Malformations: Presented by Khushveer KaurKataria DavinNoch keine Bewertungen
- Unit 8 Drugs Acting On The Endocrine SystemDokument26 SeitenUnit 8 Drugs Acting On The Endocrine SystemTherese Margarette SantiagoNoch keine Bewertungen
- AnorectalmalformationDokument126 SeitenAnorectalmalformationNinaNoch keine Bewertungen
- Milk FeverDokument10 SeitenMilk FeverMorad Imad100% (1)
- Neonatal Hypoglycemia in PigsDokument10 SeitenNeonatal Hypoglycemia in Pigssum100% (3)
- CTG Booklet: A Quick Reference Guide For Managing CtgsDokument16 SeitenCTG Booklet: A Quick Reference Guide For Managing Ctgscirlce:twoworldsconnectedNoch keine Bewertungen
- Giardia PPT M.SC Medical 4th SemDokument16 SeitenGiardia PPT M.SC Medical 4th SemRahul ChaudharyNoch keine Bewertungen
- Classification and Dosage of Antimicrobial Agents in Veterinary MedicineDokument24 SeitenClassification and Dosage of Antimicrobial Agents in Veterinary MedicineSunil0% (1)
- Cord Presentation ProlapseDokument10 SeitenCord Presentation ProlapseJHONESSA LAYOSNoch keine Bewertungen
- Cs On TefDokument10 SeitenCs On TefArchana SahuNoch keine Bewertungen
- Infantile Hypertrophic Pyloric Stenosis (IHPS) : IncidenceDokument9 SeitenInfantile Hypertrophic Pyloric Stenosis (IHPS) : IncidenceRaed AlhnaityNoch keine Bewertungen
- 2antenatal CareDokument10 Seiten2antenatal CareuouoNoch keine Bewertungen
- Antenatal Case SheetDokument4 SeitenAntenatal Case SheetRichard SnellNoch keine Bewertungen
- Lie PresentationDokument31 SeitenLie PresentationHema Malini100% (1)
- Testicular TorsionDokument20 SeitenTesticular TorsionDarshan SinghNoch keine Bewertungen
- Female External GenitaliaDokument9 SeitenFemale External Genitaliabuhari rabiuNoch keine Bewertungen
- Food Hygiene: Presentationby:-Nikita Jangra Roll No.01 2Nd Year BSC Nursing College of Nursing DR - RML HospitalDokument29 SeitenFood Hygiene: Presentationby:-Nikita Jangra Roll No.01 2Nd Year BSC Nursing College of Nursing DR - RML HospitalNikita JangraNoch keine Bewertungen
- Pyloric StenosisDokument14 SeitenPyloric Stenosisgangguan hepatobilierNoch keine Bewertungen
- Amoeboid ProtozoaDokument33 SeitenAmoeboid ProtozoaGangadharKasinathSastryNoch keine Bewertungen
- Amniotic Fluid Physiology Chemical CompositionDokument5 SeitenAmniotic Fluid Physiology Chemical CompositionMichelle San Miguel FeguroNoch keine Bewertungen
- MalariaDokument42 SeitenMalariaNiraj Kumar100% (1)
- Lecture 17 Canine InfertilityDokument28 SeitenLecture 17 Canine InfertilitygnpobsNoch keine Bewertungen
- Maternal and Perinatal Outcome in Jaundice Complicating PregnancyDokument10 SeitenMaternal and Perinatal Outcome in Jaundice Complicating PregnancymanognaaaaNoch keine Bewertungen
- Presented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Dokument19 SeitenPresented By-: Dr. Prabhata Kumar Parida ADM - No. 06ARGO/13Krushna krupa PradhanNoch keine Bewertungen
- Nutritional Causes of Infertility in Dairy CowsDokument7 SeitenNutritional Causes of Infertility in Dairy CowsReny Purnama HadiNoch keine Bewertungen
- Neonatal Hypoglycemia September 2022Dokument30 SeitenNeonatal Hypoglycemia September 2022f.abrahamNoch keine Bewertungen
- CBSE PWD EXAM Notification 2017Dokument10 SeitenCBSE PWD EXAM Notification 2017Disability Rights AllianceNoch keine Bewertungen
- 4-Systematic Surgery Abdominal HerniaDokument44 Seiten4-Systematic Surgery Abdominal HerniaabdisamedNoch keine Bewertungen
- Hiatal Hernia: BY MR, Vinay KumarDokument27 SeitenHiatal Hernia: BY MR, Vinay KumarVinay KumarNoch keine Bewertungen
- Breech PresentationDokument85 SeitenBreech Presentationwidya vannesaNoch keine Bewertungen
- Anestrus in Dairy CattleDokument43 SeitenAnestrus in Dairy CattleSuraj_Subedi88% (16)
- Pyloric StenosisDokument2 SeitenPyloric Stenosisgeorgeloto12Noch keine Bewertungen
- Cesarean Sections in CowsDokument29 SeitenCesarean Sections in CowsMădălina PodeNoch keine Bewertungen
- Ectopic Pregnancy: DR .Urmila KarkiDokument27 SeitenEctopic Pregnancy: DR .Urmila KarkiBasudev chNoch keine Bewertungen
- Post Natal CareDokument94 SeitenPost Natal CareZekariyas MulunehNoch keine Bewertungen
- Fertilisation Implantation NotesDokument4 SeitenFertilisation Implantation NotesShaun JinNoch keine Bewertungen
- 6th Cystic Ovarian DiseaseDokument15 Seiten6th Cystic Ovarian DiseaseUsama RajpootNoch keine Bewertungen
- Basic Meat Processing ProceduresDokument2 SeitenBasic Meat Processing ProceduresAbhinav Gupta100% (1)
- Embryo Transfer TechnologyDokument5 SeitenEmbryo Transfer TechnologyAbhinav GuptaNoch keine Bewertungen
- New Doc 2020-09-25 17.47.26Dokument2 SeitenNew Doc 2020-09-25 17.47.26Abhinav GuptaNoch keine Bewertungen
- Classification of Low Risk and High Risk Materials Generated in An Abattoir and Its Hygenic DisposalDokument6 SeitenClassification of Low Risk and High Risk Materials Generated in An Abattoir and Its Hygenic DisposalAbhinav GuptaNoch keine Bewertungen
- Abattoir Design and Construction PDFDokument4 SeitenAbattoir Design and Construction PDFAbhinav Gupta100% (2)
- Egg Notes LPT 3rd Yr BVSCDokument7 SeitenEgg Notes LPT 3rd Yr BVSCAbhinav GuptaNoch keine Bewertungen
- Sulphonamides PDFDokument11 SeitenSulphonamides PDFAbhinav GuptaNoch keine Bewertungen
- Agrochemicals Toxicity PDFDokument14 SeitenAgrochemicals Toxicity PDFAbhinav GuptaNoch keine Bewertungen
- Horse Vs Cattle Meat, Sheep Vs Goat MeatDokument4 SeitenHorse Vs Cattle Meat, Sheep Vs Goat MeatAbhinav GuptaNoch keine Bewertungen
- Pharmacology - 2. Unit 01. New - HighlightedDokument4 SeitenPharmacology - 2. Unit 01. New - HighlightedManish ShankarpureNoch keine Bewertungen
- Arsenic ToxicityDokument11 SeitenArsenic ToxicityAbhinav GuptaNoch keine Bewertungen
- Nitrite and Chlorate ToxicityDokument11 SeitenNitrite and Chlorate ToxicityAbhinav GuptaNoch keine Bewertungen
- Fluorine Toxicity, Common Salt and Urea PoisoningDokument21 SeitenFluorine Toxicity, Common Salt and Urea PoisoningAbhinav GuptaNoch keine Bewertungen
- Histamine and Antihistamines. NotesDokument5 SeitenHistamine and Antihistamines. NotesSubha2000100% (1)
- Agrochemicals Toxicity PDFDokument14 SeitenAgrochemicals Toxicity PDFAbhinav GuptaNoch keine Bewertungen
- Arawali Veterinary College: Department of Livestock Production TechnologyDokument19 SeitenArawali Veterinary College: Department of Livestock Production TechnologyAbhinav GuptaNoch keine Bewertungen
- LPT Assignment For 2nd Internal AssessmentDokument4 SeitenLPT Assignment For 2nd Internal AssessmentAbhinav GuptaNoch keine Bewertungen
- Table Poultry AMIDokument2 SeitenTable Poultry AMIAbhinav GuptaNoch keine Bewertungen
- Animal Husbandry PaperDokument6 SeitenAnimal Husbandry PaperAbhinav GuptaNoch keine Bewertungen
- New Microsoft Office Word DocumentDokument45 SeitenNew Microsoft Office Word DocumentAbhinav GuptaNoch keine Bewertungen
- Milk PropertiesDokument18 SeitenMilk PropertiesAbhinav GuptaNoch keine Bewertungen
- Milk Hygiene Practice in IndiaDokument4 SeitenMilk Hygiene Practice in IndiaAbhinav GuptaNoch keine Bewertungen
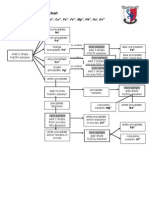
- Speciation of MeatDokument21 SeitenSpeciation of MeatAbhinav GuptaNoch keine Bewertungen
- Role of VetDokument4 SeitenRole of VetAbhinav GuptaNoch keine Bewertungen
- Milk Hygiene Practice in IndiaDokument4 SeitenMilk Hygiene Practice in IndiaAbhinav GuptaNoch keine Bewertungen
- Milk Hygiene Practice in IndiaDokument4 SeitenMilk Hygiene Practice in IndiaAbhinav GuptaNoch keine Bewertungen
- Maximum Residue Levels For Common AnthelminticsDokument2 SeitenMaximum Residue Levels For Common AnthelminticsAbhinav GuptaNoch keine Bewertungen
- Milk Processing 10000 LPDDokument29 SeitenMilk Processing 10000 LPDLATHWALBRONoch keine Bewertungen
- Classification of Low Risk and High Risk Materials Generated in An Abattoir and Its Hygenic DisposalDokument6 SeitenClassification of Low Risk and High Risk Materials Generated in An Abattoir and Its Hygenic DisposalAbhinav GuptaNoch keine Bewertungen
- 200mm 250mm 300 MM: Project Name Location Bill No. - 00 (Rev. 0) Consultant Contractor Buildiong Name DATEDokument2 Seiten200mm 250mm 300 MM: Project Name Location Bill No. - 00 (Rev. 0) Consultant Contractor Buildiong Name DATEganesh gundNoch keine Bewertungen
- Polycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentDokument19 SeitenPolycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentAkshay HarekarNoch keine Bewertungen
- Allowable Stresses of Typical ASME Materials - Stainless SteelDokument5 SeitenAllowable Stresses of Typical ASME Materials - Stainless SteelChanchal K SankaranNoch keine Bewertungen
- Juri Ferrer - Ws - WeatherDokument4 SeitenJuri Ferrer - Ws - WeathersJIqsNoch keine Bewertungen
- Vertical Transportation in BuildingsDokument46 SeitenVertical Transportation in BuildingsHIMA MiniNoch keine Bewertungen
- Grade 10 Chemistry Week 1Dokument3 SeitenGrade 10 Chemistry Week 1Nikoli MajorNoch keine Bewertungen
- All Electricity Worksheets For Midterm 22Dokument22 SeitenAll Electricity Worksheets For Midterm 22Maryam AlkaabiNoch keine Bewertungen
- ISO 9001 Required DocumentationDokument3 SeitenISO 9001 Required Documentationdnmule100% (1)
- Punjab National BankDokument4 SeitenPunjab National BankShubham RajNoch keine Bewertungen
- Final Workshop Report On Value Addition and AgroprocessingDokument31 SeitenFinal Workshop Report On Value Addition and AgroprocessingBett K. BernardNoch keine Bewertungen
- Testing For Cations Flow ChartDokument2 SeitenTesting For Cations Flow Chartapi-252561013Noch keine Bewertungen
- Bars Performance AppraisalDokument6 SeitenBars Performance AppraisalPhillip Miler0% (1)
- AFC Refereeing Fitness Training Guidelines - FinalDokument42 SeitenAFC Refereeing Fitness Training Guidelines - FinalAPH FARM BONDOWOSONoch keine Bewertungen
- MUMMY'S KITCHEN NEW FinalDokument44 SeitenMUMMY'S KITCHEN NEW Finalanon_602671575100% (4)
- Quorum Sensing PDFDokument9 SeitenQuorum Sensing PDFShareenMuneebNoch keine Bewertungen
- GAD OrientationDokument58 SeitenGAD OrientationKevin Dalangin100% (2)
- Weaning Guidelines 2007Dokument4 SeitenWeaning Guidelines 2007deliejoyceNoch keine Bewertungen
- 6 Instrumentation PDFDokument144 Seiten6 Instrumentation PDFWanderley MandruzatoNoch keine Bewertungen
- Fosroc Conplast SP335: Multi-Range Water Reducing AdmixtureDokument2 SeitenFosroc Conplast SP335: Multi-Range Water Reducing AdmixtureVincent JavateNoch keine Bewertungen
- Bai Tap Anh 9 Tuan 19202122 - 2032023135013Dokument21 SeitenBai Tap Anh 9 Tuan 19202122 - 2032023135013Duy HoangNoch keine Bewertungen
- Flock MenuDokument5 SeitenFlock MenuWilson TayNoch keine Bewertungen
- Formula Sheet Pre-MidDokument4 SeitenFormula Sheet Pre-MidUzair KhanNoch keine Bewertungen
- World Wide Emission Free E-Motercycle ProjectDokument20 SeitenWorld Wide Emission Free E-Motercycle ProjectAkshay SharmaNoch keine Bewertungen
- Lead in Water: Standard Test Methods ForDokument17 SeitenLead in Water: Standard Test Methods ForAMMARNoch keine Bewertungen
- References: ProblemsDokument14 SeitenReferences: ProblemsDiego AlejandroNoch keine Bewertungen
- Zook Rupture Disc URADokument2 SeitenZook Rupture Disc URAmd_taheriNoch keine Bewertungen
- Alcohol Consumption and Related Crime Incident in John Paul CollegeDokument17 SeitenAlcohol Consumption and Related Crime Incident in John Paul Collegejoy mesanaNoch keine Bewertungen
- API 16C ErrataDokument1 SeiteAPI 16C ErrataDinesh KumarNoch keine Bewertungen
- Fourier Ptychography Stivi ElbiDokument20 SeitenFourier Ptychography Stivi ElbistiviNoch keine Bewertungen
- Mechanism of Enzyme ActionDokument19 SeitenMechanism of Enzyme ActionRubi AnnNoch keine Bewertungen