Das könnte Ihnen auch gefallen
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesVon EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNoch keine Bewertungen
- Angina Pectoris and Atherosclerotic Risk Factors in The MultisiteDokument8 SeitenAngina Pectoris and Atherosclerotic Risk Factors in The Multisiteger4ld1nNoch keine Bewertungen
- Populasi 12Dokument4 SeitenPopulasi 12Resky Ika Sah PutriNoch keine Bewertungen
- Module 4Dokument35 SeitenModule 4latifaNoch keine Bewertungen
- Once-Weekly Semaglutide in Adults With Overweight or ObesityDokument34 SeitenOnce-Weekly Semaglutide in Adults With Overweight or ObesityRIJO CHERIANNoch keine Bewertungen
- Interactive Video Dance Games For Healthy Older Adults 2010Dokument3 SeitenInteractive Video Dance Games For Healthy Older Adults 2010LilianaRodríguezNoch keine Bewertungen
- The Efficacy of A 9-Month Treadmill Walking Program On The Exercise Capacity and Weight Reduction For Adolescents With Severe AutismDokument10 SeitenThe Efficacy of A 9-Month Treadmill Walking Program On The Exercise Capacity and Weight Reduction For Adolescents With Severe AutismmarikosvaNoch keine Bewertungen
- The Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorDokument6 SeitenThe Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorIJPHSNoch keine Bewertungen
- Health Believes and OsteoporosisDokument31 SeitenHealth Believes and OsteoporosistarikeopsNoch keine Bewertungen
- EnergiDokument9 SeitenEnergiAnonymous LjInbcyP4Noch keine Bewertungen
- Correlation of Perceived Stress and GI Symptoms in Medical Students in OmanDokument6 SeitenCorrelation of Perceived Stress and GI Symptoms in Medical Students in OmanajmrdNoch keine Bewertungen
- A Study On Health Seeking Behavior Among Married Reproductive Age Group Women in A Rural AreaDokument4 SeitenA Study On Health Seeking Behavior Among Married Reproductive Age Group Women in A Rural AreasupriaprNoch keine Bewertungen
- Five Times Sit To Stand (5Tsts) : InstructionsDokument2 SeitenFive Times Sit To Stand (5Tsts) : InstructionsNovinna KusumawatiNoch keine Bewertungen
- Sjams 26F3307 3314 PDFDokument8 SeitenSjams 26F3307 3314 PDFnaveenNoch keine Bewertungen
- Associations of Physical Activity and Depression Results From The IrishDokument8 SeitenAssociations of Physical Activity and Depression Results From The IrishHargo PsyNoch keine Bewertungen
- Maughan Et Al. (2012) PDFDokument15 SeitenMaughan Et Al. (2012) PDFvabrandaoNoch keine Bewertungen
- Cancers 12 03000Dokument13 SeitenCancers 12 03000Gary LheureuxNoch keine Bewertungen
- Effectiveness of Acceptance and Commitment Therapy On Weight, Eating Behaviours and Psychological Outcomes A Systematic Review and Meta-AnalysisDokument13 SeitenEffectiveness of Acceptance and Commitment Therapy On Weight, Eating Behaviours and Psychological Outcomes A Systematic Review and Meta-AnalysisAna Gómez EstebanNoch keine Bewertungen
- Regis Class of 2009 AOP ComorbiditiesDokument24 SeitenRegis Class of 2009 AOP ComorbiditiesTim Noteboom100% (1)
- Halliday 2018Dokument4 SeitenHalliday 2018Fadhli Fadhlial faruqNoch keine Bewertungen
- Effect of Physical Activity On Cognition and Daily Living Activities of The Elderly With Mild DementiaDokument6 SeitenEffect of Physical Activity On Cognition and Daily Living Activities of The Elderly With Mild DementiaMahfilza MayubNoch keine Bewertungen
- 6 Minute Walk TestDokument7 Seiten6 Minute Walk Testriccardo6grassiNoch keine Bewertungen
- Analysis of Blood PressureDokument18 SeitenAnalysis of Blood PressureYessy KurniatiNoch keine Bewertungen
- Gait Speed and Survival JAMA 2011Dokument9 SeitenGait Speed and Survival JAMA 2011Priscila DanieleNoch keine Bewertungen
- Effects of Stationary Cycling Exercise On The Balance and Gait Abilities of Chronic Stroke PatientsDokument3 SeitenEffects of Stationary Cycling Exercise On The Balance and Gait Abilities of Chronic Stroke PatientsJhonnyNogueraNoch keine Bewertungen
- Art 228Dokument5 SeitenArt 228Antoanela OlteanNoch keine Bewertungen
- 2009 Malawi FactSheet enDokument2 Seiten2009 Malawi FactSheet enchiradzuluNoch keine Bewertungen
- SAP Ca. MamaeDokument6 SeitenSAP Ca. Mamaetasya siti murbaraniNoch keine Bewertungen
- Muscular and Functional Capacity in Subjects Under TreatmentDokument7 SeitenMuscular and Functional Capacity in Subjects Under Treatmentdavid fernandezNoch keine Bewertungen
- Hiperbar O2Dokument22 SeitenHiperbar O2Zekany AndreiNoch keine Bewertungen
- Results of The Physical Rehabilitation of Patients With Pulmonary TuberculosisDokument7 SeitenResults of The Physical Rehabilitation of Patients With Pulmonary Tuberculosisnur fajri rahmiNoch keine Bewertungen
- 01 Mss 0000536104 89809 d8Dokument1 Seite01 Mss 0000536104 89809 d8Iyappan SubramaniNoch keine Bewertungen
- Health Status of Elderly Based On Daily Activities Living, Cholesterol and Uric Acid Profile in Medan CityDokument6 SeitenHealth Status of Elderly Based On Daily Activities Living, Cholesterol and Uric Acid Profile in Medan CityYolanda Olivia SinagaNoch keine Bewertungen
- The Benefits of Custom Exergames For Fitness, Balance, and Health-Related Quality of Life: A Randomized Controlled Trial With Community-Dwelling Older AdultsDokument9 SeitenThe Benefits of Custom Exergames For Fitness, Balance, and Health-Related Quality of Life: A Randomized Controlled Trial With Community-Dwelling Older AdultsAnonymous HUY0yRexYfNoch keine Bewertungen
- Osmani+and+Peric+MS85+ (60 79)Dokument20 SeitenOsmani+and+Peric+MS85+ (60 79)nourelyakine.lakhdarNoch keine Bewertungen
- Aartolahti2020 Article Long-termStrengthAndBalanceTraDokument8 SeitenAartolahti2020 Article Long-termStrengthAndBalanceTraLucasNoch keine Bewertungen
- Fueling The Obesity Epidemic Artificially Sweetened BeveragesDokument7 SeitenFueling The Obesity Epidemic Artificially Sweetened BeveragesJOCELYN ACEVEDONoch keine Bewertungen
- Physical Activity Index of Female U StudentsDokument4 SeitenPhysical Activity Index of Female U Studentsنور امالينا زاينونNoch keine Bewertungen
- Articulo Unsa V5Dokument21 SeitenArticulo Unsa V5English RoomNoch keine Bewertungen
- Samuthpongtorn 2023 LD 230182 1694535872.81978Dokument4 SeitenSamuthpongtorn 2023 LD 230182 1694535872.81978bgx67nnnkgNoch keine Bewertungen
- Risk Factors of Osteoarthritis Knee - A Cross-Sectional StudyDokument3 SeitenRisk Factors of Osteoarthritis Knee - A Cross-Sectional StudyElias Oktovianus HaulussyNoch keine Bewertungen
- Pergamon 0005-7967 (94) 00070-0: (Received 29 June 1994)Dokument5 SeitenPergamon 0005-7967 (94) 00070-0: (Received 29 June 1994)Aggelou MayaNoch keine Bewertungen
- Role of Caregivers' Burden On Qol of DiabeticsDokument17 SeitenRole of Caregivers' Burden On Qol of DiabeticsMarufat OdetundeNoch keine Bewertungen
- 285-Article Text-1751-1-10-20210728Dokument12 Seiten285-Article Text-1751-1-10-20210728Bimo AnggoroNoch keine Bewertungen
- 1 s2.0 S1836955315001174 MainDokument1 Seite1 s2.0 S1836955315001174 MainVicky VigneshNoch keine Bewertungen
- Quality of Life of Laryngeal Carcinoma Patients After Total LaryngectomyDokument13 SeitenQuality of Life of Laryngeal Carcinoma Patients After Total LaryngectomySelvi Puspa SariNoch keine Bewertungen
- Ffects of Small-Sided Recreational Volleyball On: E Health Markers and Physical Fitness in Middle-Aged MenDokument10 SeitenFfects of Small-Sided Recreational Volleyball On: E Health Markers and Physical Fitness in Middle-Aged MenJAN GUZMANNoch keine Bewertungen
- Toxins 12 00420 v3Dokument11 SeitenToxins 12 00420 v3Carlos Miguel Mendoza LlamocaNoch keine Bewertungen
- Archives of Gerontology and GeriatricsDokument7 SeitenArchives of Gerontology and GeriatricsBimo AnggoroNoch keine Bewertungen
- ENEA PosterDokument6 SeitenENEA PosterPrudwiraj SanamandraNoch keine Bewertungen
- 14 - Results and Discussion PDFDokument62 Seiten14 - Results and Discussion PDFAman ShrivastavaNoch keine Bewertungen
- Individual Perceptions of Adolescents in Efforts To Prevent HypertensionDokument4 SeitenIndividual Perceptions of Adolescents in Efforts To Prevent HypertensionNikmatul fadilahNoch keine Bewertungen
- 1569 3921 1 SM PDFDokument12 Seiten1569 3921 1 SM PDFWening HapsariNoch keine Bewertungen
- Jurnal AT LianDokument8 SeitenJurnal AT LianliankaigereNoch keine Bewertungen
- Kapetanakis 2017Dokument7 SeitenKapetanakis 2017Rvo ProductionNoch keine Bewertungen
- Research Article: The Effects of Exercise On The Physical Fitness of High and Moderate-Low Functioning Older Adult WomenDokument7 SeitenResearch Article: The Effects of Exercise On The Physical Fitness of High and Moderate-Low Functioning Older Adult WomenabcsouzaNoch keine Bewertungen
- Sensorimotor Training For BalanceDokument7 SeitenSensorimotor Training For BalanceAgatha SharmaNoch keine Bewertungen
- Socio-Demography, Nutritional Status and Physical Activity Among Elderly in Samarahan Division, Sarawak, Malaysia9-39480-1-ED (EDIT C)Dokument7 SeitenSocio-Demography, Nutritional Status and Physical Activity Among Elderly in Samarahan Division, Sarawak, Malaysia9-39480-1-ED (EDIT C)IJPHSNoch keine Bewertungen
- Assessment of Health-Related Quality of Life Among Patients With Non-Communicable DiseasesDokument6 SeitenAssessment of Health-Related Quality of Life Among Patients With Non-Communicable DiseasesIJPHSNoch keine Bewertungen
- December 3rd Parish Newsletter 2023Dokument2 SeitenDecember 3rd Parish Newsletter 2023John HayesNoch keine Bewertungen
- Portarlington Parish Newsletter APRIL 30th 2023 - Fourth Sunday of EasterDokument2 SeitenPortarlington Parish Newsletter APRIL 30th 2023 - Fourth Sunday of EasterJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter August 27th - Twenty First Sunday in O.T PDFDokument2 SeitenPortarlington Parish Newsletter August 27th - Twenty First Sunday in O.T PDFJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter July 16th 2023 - Fifteenth Sunday in o TDokument2 SeitenPortarlington Parish Newsletter July 16th 2023 - Fifteenth Sunday in o TJohn HayesNoch keine Bewertungen
- September 3rd - Twenty Second Sunday in O.T. - Parish Newsletter PDFDokument2 SeitenSeptember 3rd - Twenty Second Sunday in O.T. - Parish Newsletter PDFJohn HayesNoch keine Bewertungen
- APRIL 23rd 2023 - Third Sunday of Easter - Parish Newsletter PDFDokument2 SeitenAPRIL 23rd 2023 - Third Sunday of Easter - Parish Newsletter PDFJohn HayesNoch keine Bewertungen
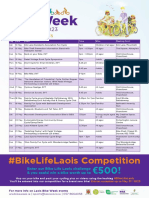
- LCC Bike Week A4 GENERAL Events List 2023Dokument1 SeiteLCC Bike Week A4 GENERAL Events List 2023John HayesNoch keine Bewertungen
- Threshold We Are Gen Rent 2023Dokument56 SeitenThreshold We Are Gen Rent 2023John HayesNoch keine Bewertungen
- Portarlington Parish Newsletter MAY 14TH 2023 - Sixth Sunday of EasterDokument2 SeitenPortarlington Parish Newsletter MAY 14TH 2023 - Sixth Sunday of EasterJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter MAY 21st 2023 - Ascension of The LordDokument2 SeitenPortarlington Parish Newsletter MAY 21st 2023 - Ascension of The LordJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter February 19thDokument2 SeitenPortarlington Parish Newsletter February 19thJohn HayesNoch keine Bewertungen
- Kolbe School UpdateDokument2 SeitenKolbe School UpdateJohn HayesNoch keine Bewertungen
- Signed Results Sheet For Portlaoise LEADokument2 SeitenSigned Results Sheet For Portlaoise LEAJohn HayesNoch keine Bewertungen
- April 16th - Divine Mercy Sunday Second Sunday Easter 2023 - Parish NewsletterDokument2 SeitenApril 16th - Divine Mercy Sunday Second Sunday Easter 2023 - Parish NewsletterJohn HayesNoch keine Bewertungen
- March 12th 3rd Sunday of Lent 2023 Parish NewsletterDokument2 SeitenMarch 12th 3rd Sunday of Lent 2023 Parish NewsletterJohn HayesNoch keine Bewertungen
- March 19th - 4th Sunday of Lent 2023 Parish Newsletter PDFDokument2 SeitenMarch 19th - 4th Sunday of Lent 2023 Parish Newsletter PDFJohn HayesNoch keine Bewertungen
- National Cultivate Week 2023Dokument1 SeiteNational Cultivate Week 2023John HayesNoch keine Bewertungen
- April 2nd - Palm Sunday 2023 - Portarlington Parish NewsletterDokument2 SeitenApril 2nd - Palm Sunday 2023 - Portarlington Parish NewsletterJohn HayesNoch keine Bewertungen
- Portarlington Parish February 12th Parish NewsletterDokument2 SeitenPortarlington Parish February 12th Parish NewsletterJohn HayesNoch keine Bewertungen
- February 26th 1st Sunday of Lent 2023 Parish Newsletter PDFDokument2 SeitenFebruary 26th 1st Sunday of Lent 2023 Parish Newsletter PDFJohn HayesNoch keine Bewertungen
- March 5th 2nd Sunday of Lent 2023 Parish Newsletter PDFDokument2 SeitenMarch 5th 2nd Sunday of Lent 2023 Parish Newsletter PDFJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter Parish NewsletterDokument2 SeitenPortarlington Parish Newsletter Parish NewsletterJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter January 8thDokument2 SeitenPortarlington Parish Newsletter January 8thJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter January 29th NewsletterDokument2 SeitenPortarlington Parish Newsletter January 29th NewsletterJohn HayesNoch keine Bewertungen
- Laois GAA Handball Review of The Year 2022Dokument16 SeitenLaois GAA Handball Review of The Year 2022John HayesNoch keine Bewertungen
- Portarlington Parish Newsletter January 15th PDFDokument2 SeitenPortarlington Parish Newsletter January 15th PDFJohn HayesNoch keine Bewertungen
- Portarlington Parish Newsletter December 18th 2022 - Fourth Sunday of Advent Newsletter PDFDokument2 SeitenPortarlington Parish Newsletter December 18th 2022 - Fourth Sunday of Advent Newsletter PDFJohn HayesNoch keine Bewertungen
- Portarlington Parish January 22nd NewsletterDokument2 SeitenPortarlington Parish January 22nd NewsletterJohn HayesNoch keine Bewertungen
- Map of Property Clara CO. Offaly 2022Dokument1 SeiteMap of Property Clara CO. Offaly 2022John HayesNoch keine Bewertungen
- Portarlington Parish Newsletter December 25th 2022Dokument2 SeitenPortarlington Parish Newsletter December 25th 2022John HayesNoch keine Bewertungen
- Architectural Design I: SyllabusDokument3 SeitenArchitectural Design I: SyllabusSrilakshmi PriyaNoch keine Bewertungen
- Food Safety Plan of Catalonia: GuidelinesDokument38 SeitenFood Safety Plan of Catalonia: GuidelinesralapubsNoch keine Bewertungen
- The Example of Text That Contains Present Perfect TenseDokument2 SeitenThe Example of Text That Contains Present Perfect TenseRahmiSyariif100% (1)
- The Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentDokument4 SeitenThe Effectiveness of Peppermint Oil (Mentha X Pepipirita) As Mosquito RepellentKester PlaydaNoch keine Bewertungen
- Script - Macbeth A La MafiosiDokument27 SeitenScript - Macbeth A La MafiosiMohd Afiq Mat RazaiNoch keine Bewertungen
- Instrumentation. Between Science, State and IndustryDokument271 SeitenInstrumentation. Between Science, State and IndustryMichel GautamaNoch keine Bewertungen
- Group 4 CariCRIS Case SubmissionDokument6 SeitenGroup 4 CariCRIS Case SubmissionKingsuk MaityNoch keine Bewertungen
- CO - Config Sap Top JobsDokument81 SeitenCO - Config Sap Top JobsAditya PakalaNoch keine Bewertungen
- Reading Activity - A Lost DogDokument3 SeitenReading Activity - A Lost DogGigsFloripaNoch keine Bewertungen
- 10 Applications in Engineering Mechanics PDFDokument10 Seiten10 Applications in Engineering Mechanics PDFWolf Lord100% (1)
- DataSheet CertificationPaths InsuranceSuite AnalystsDokument7 SeitenDataSheet CertificationPaths InsuranceSuite Analystsshanmuga89Noch keine Bewertungen
- Lecture - 4 - 28june2023Dokument18 SeitenLecture - 4 - 28june2023vanshikaNoch keine Bewertungen
- Adh Dialectical JournalDokument4 SeitenAdh Dialectical Journalapi-521174998Noch keine Bewertungen
- Teresa of Avila - The Life of ST Teresa, A Carmelite Nun Reprint 1912Dokument674 SeitenTeresa of Avila - The Life of ST Teresa, A Carmelite Nun Reprint 1912WaterwindNoch keine Bewertungen
- Chapter 1Dokument13 SeitenChapter 1Jerard AnciroNoch keine Bewertungen
- Figures of Speech StylisticsDokument11 SeitenFigures of Speech StylisticsCarmie Lactaotao DasallaNoch keine Bewertungen
- Sampling Strategies For Heterogeneous WastesDokument18 SeitenSampling Strategies For Heterogeneous Wastesmohammed karasnehNoch keine Bewertungen
- Coursera Qs-Ans For Financial AidDokument2 SeitenCoursera Qs-Ans For Financial AidMarno03Noch keine Bewertungen
- HRM848 Training Techniques and Practices Summer 2021Dokument39 SeitenHRM848 Training Techniques and Practices Summer 2021Dhruvi RajNoch keine Bewertungen
- STRUCTURAL CONVERSION Examples PDFDokument5 SeitenSTRUCTURAL CONVERSION Examples PDFGerard Salmoral ParramonNoch keine Bewertungen
- Gein, EdDokument10 SeitenGein, Edpetru_k1Noch keine Bewertungen
- Bayonet Charge Vs ExposureDokument2 SeitenBayonet Charge Vs ExposureДжейнушка ПаннеллNoch keine Bewertungen
- Tapan Pathak Case StudiesDokument33 SeitenTapan Pathak Case StudiesNeelee SoniNoch keine Bewertungen
- A Vagabond SongDokument4 SeitenA Vagabond SongLiLiana DewiNoch keine Bewertungen
- New-Product Development and Product Life-Cycle Strategies GENERAL CONTENT: Multiple-Choice QuestionsDokument21 SeitenNew-Product Development and Product Life-Cycle Strategies GENERAL CONTENT: Multiple-Choice Questionslisa voNoch keine Bewertungen
- Gender Stereotypes and Performativity Analysis in Norwegian Wood Novel by Haruki Murakami Devani Adinda Putri Reg No: 2012060541Dokument35 SeitenGender Stereotypes and Performativity Analysis in Norwegian Wood Novel by Haruki Murakami Devani Adinda Putri Reg No: 2012060541Jornel JevanskiNoch keine Bewertungen
- Constitution & By-LawsDokument15 SeitenConstitution & By-LawsMichael C. AndradeNoch keine Bewertungen
- News StoryDokument1 SeiteNews StoryRic Anthony LayasanNoch keine Bewertungen
- ATHE Level 3 Diploma in Business (RQF / 60 Credits)Dokument4 SeitenATHE Level 3 Diploma in Business (RQF / 60 Credits)GibsonNoch keine Bewertungen
- AZ-300 - Azure Solutions Architect TechnologiesDokument3 SeitenAZ-300 - Azure Solutions Architect TechnologiesAmar Singh100% (1)