Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Lenovo S340-15iwl Compal LA-H101P SchematicDokument53 SeitenLenovo S340-15iwl Compal LA-H101P SchematicYetawa Guaviare100% (4)
- LhiannanDokument6 SeitenLhiannanGreybornNoch keine Bewertungen
- B1 Editable End-of-Year TestDokument6 SeitenB1 Editable End-of-Year TestSyahira Mayadi50% (2)
- Evidence Based Practice in Nursing Healthcare A Guide To Best Practice 3rd Edition Ebook PDFDokument62 SeitenEvidence Based Practice in Nursing Healthcare A Guide To Best Practice 3rd Edition Ebook PDFwilliam.tavares69198% (50)
- Tourism and GastronomyDokument245 SeitenTourism and GastronomySakurel ZenzeiNoch keine Bewertungen
- Detailed Lesson Plan in Mathematics (Pythagorean Theorem)Dokument6 SeitenDetailed Lesson Plan in Mathematics (Pythagorean Theorem)Carlo DascoNoch keine Bewertungen
- #Healthatwork: Tweetreach Report ForDokument16 Seiten#Healthatwork: Tweetreach Report ForNational Healthcare Decisions DayNoch keine Bewertungen
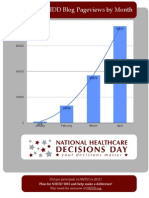
- NHDD by The Numbers: Blog Page ViewsDokument1 SeiteNHDD by The Numbers: Blog Page ViewsNational Healthcare Decisions DayNoch keine Bewertungen
- NHDD 2012 Twitter ImpressionsDokument13 SeitenNHDD 2012 Twitter ImpressionsNational Healthcare Decisions DayNoch keine Bewertungen
- Letter To President ObamaDokument4 SeitenLetter To President ObamaNational Healthcare Decisions DayNoch keine Bewertungen
- Power of Attorney Form (NM DDPC)Dokument6 SeitenPower of Attorney Form (NM DDPC)National Healthcare Decisions DayNoch keine Bewertungen
- Mental Health Treatment Advance Directive-Optional (NM DDPC)Dokument6 SeitenMental Health Treatment Advance Directive-Optional (NM DDPC)National Healthcare Decisions DayNoch keine Bewertungen
- ER Packet - Laminated Card Re Advance Directives - NM DDPC ResourceDokument2 SeitenER Packet - Laminated Card Re Advance Directives - NM DDPC ResourceNational Healthcare Decisions DayNoch keine Bewertungen
- New Mexico ProclamationDokument1 SeiteNew Mexico ProclamationNational Healthcare Decisions DayNoch keine Bewertungen
- More Americans Discussing - and Planning - TreatmentDokument45 SeitenMore Americans Discussing - and Planning - TreatmentNational Healthcare Decisions DayNoch keine Bewertungen
- Brief Communication & Living WillsDokument6 SeitenBrief Communication & Living WillsNational Healthcare Decisions DayNoch keine Bewertungen
- NHDD Case StatementDokument2 SeitenNHDD Case StatementNational Healthcare Decisions DayNoch keine Bewertungen
- AHRQ Research in Action: Advance Care PlanningDokument20 SeitenAHRQ Research in Action: Advance Care PlanningNational Healthcare Decisions DayNoch keine Bewertungen
- Tweetreach For #Havethetalk: Reached ViaDokument8 SeitenTweetreach For #Havethetalk: Reached ViaNational Healthcare Decisions DayNoch keine Bewertungen
- TweetReach - Decisions - Day 2010Dokument35 SeitenTweetReach - Decisions - Day 2010National Healthcare Decisions DayNoch keine Bewertungen
- Dr. Babasaheb Ambedkar Technological UniversityDokument3 SeitenDr. Babasaheb Ambedkar Technological UniversityalfajNoch keine Bewertungen
- Datasheet of STS 6000K H1 GCADokument1 SeiteDatasheet of STS 6000K H1 GCAHome AutomatingNoch keine Bewertungen
- Aluminium PasteDokument11 SeitenAluminium PasteGovindanayagi PattabiramanNoch keine Bewertungen
- First Aid Transportation of The InjuredDokument30 SeitenFirst Aid Transportation of The InjuredMuhammad Naveed Akhtar100% (1)
- 20150714rev1 ASPACC 2015Dokument22 Seiten20150714rev1 ASPACC 2015HERDI SUTANTONoch keine Bewertungen
- 02 Laboratory Exercise 1Dokument2 Seiten02 Laboratory Exercise 1Mico Bryan BurgosNoch keine Bewertungen
- Tech SharmitDokument16 SeitenTech SharmitRishu SinhaNoch keine Bewertungen
- INDUSTRIAL PHD POSITION - Sensor Fusion Enabled Indoor PositioningDokument8 SeitenINDUSTRIAL PHD POSITION - Sensor Fusion Enabled Indoor Positioningzeeshan ahmedNoch keine Bewertungen
- BQ - Structural Works - CompressedDokument163 SeitenBQ - Structural Works - CompressedLee YuxuanNoch keine Bewertungen
- Human Aspect Issues After Mergers and AcquisitionsDokument4 SeitenHuman Aspect Issues After Mergers and AcquisitionsA B100% (1)
- Term Paper A and CDokument9 SeitenTerm Paper A and CKishaloy NathNoch keine Bewertungen
- Duties and Responsibilities - Filipino DepartmentDokument2 SeitenDuties and Responsibilities - Filipino DepartmentEder Aguirre Capangpangan100% (2)
- 3-CHAPTER-1 - Edited v1Dokument32 Seiten3-CHAPTER-1 - Edited v1Michael Jaye RiblezaNoch keine Bewertungen
- MultiZone Limitations and HintsDokument2 SeitenMultiZone Limitations and HintsRubén Darío Becerra GalindoNoch keine Bewertungen
- DSS 2 (7th&8th) May2018Dokument2 SeitenDSS 2 (7th&8th) May2018Piara SinghNoch keine Bewertungen
- Color Coding Chart - AHGDokument3 SeitenColor Coding Chart - AHGahmedNoch keine Bewertungen
- Electromyostimulation StudyDokument22 SeitenElectromyostimulation StudyAgnes Sophia PenuliarNoch keine Bewertungen
- (Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)Dokument192 Seiten(Biophysical Techniques Series) Iain D. Campbell, Raymond A. Dwek-Biological Spectroscopy - Benjamin-Cummings Publishing Company (1984)BrunoRamosdeLima100% (1)
- How To Build Yam Chips Production PlantDokument11 SeitenHow To Build Yam Chips Production PlantVu Thieu TuanNoch keine Bewertungen
- Chapter 8 - Current Electricity - Selina Solutions Concise Physics Class 10 ICSE - KnowledgeBoatDokument123 SeitenChapter 8 - Current Electricity - Selina Solutions Concise Physics Class 10 ICSE - KnowledgeBoatskjNoch keine Bewertungen
- 7 Ways To Support Your Babys Learning Today Monti KidsDokument19 Seiten7 Ways To Support Your Babys Learning Today Monti KidsMareim A HachiNoch keine Bewertungen
- Cryptocurrency Research PDFDokument59 SeitenCryptocurrency Research PDFAnupriyaNoch keine Bewertungen
- Lesson 3 - Adaptation AssignmentDokument3 SeitenLesson 3 - Adaptation AssignmentEmmy RoseNoch keine Bewertungen
- Unix SapDokument4 SeitenUnix SapsatyavaninaiduNoch keine Bewertungen