Das könnte Ihnen auch gefallen
- of E-Aushadi FinalDokument48 Seitenof E-Aushadi Finalv_ratNoch keine Bewertungen
- Case Demand Measurement and Forecasting Block-2 Ch.4Dokument3 SeitenCase Demand Measurement and Forecasting Block-2 Ch.4v_ratNoch keine Bewertungen
- Marketing Research Chapter Case Block-2 Ch.5Dokument4 SeitenMarketing Research Chapter Case Block-2 Ch.5v_rat0% (1)
- Inv. Mgt. Procurement & DistributionDokument78 SeitenInv. Mgt. Procurement & Distributionv_ratNoch keine Bewertungen
- Drugs Store Management: Dr. Nirmal GurbaniDokument94 SeitenDrugs Store Management: Dr. Nirmal Gurbaniv_ratNoch keine Bewertungen
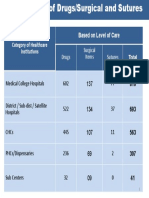
- Category of Healthcare Institutions Based On Level of Care: Drugs Surgical Items SuturesDokument1 SeiteCategory of Healthcare Institutions Based On Level of Care: Drugs Surgical Items Suturesv_ratNoch keine Bewertungen
- Access To Quality Medicines: Rajasthan Model: "Reaching The Unreached"Dokument7 SeitenAccess To Quality Medicines: Rajasthan Model: "Reaching The Unreached"v_ratNoch keine Bewertungen
- Day 4 - ReliabilityDokument11 SeitenDay 4 - Reliabilityv_ratNoch keine Bewertungen
- Quantification of Health Commodities - RMNCH SupplementDokument173 SeitenQuantification of Health Commodities - RMNCH Supplementv_ratNoch keine Bewertungen
- A Strategic Essential in Healthcare Systems OutsourcingDokument22 SeitenA Strategic Essential in Healthcare Systems Outsourcingv_ratNoch keine Bewertungen
- Day 2 - Equipment Preventive MaintenanceDokument29 SeitenDay 2 - Equipment Preventive Maintenancev_ratNoch keine Bewertungen
- Day 8 Inventory ManagementDokument56 SeitenDay 8 Inventory Managementv_ratNoch keine Bewertungen
- UNFPA RFQ QA Framework - Low - V11Dokument32 SeitenUNFPA RFQ QA Framework - Low - V11v_ratNoch keine Bewertungen
- Day 3 - Equipment Disposal, Audit, T&DDokument35 SeitenDay 3 - Equipment Disposal, Audit, T&Dv_ratNoch keine Bewertungen
- Introduction To Epidemiology: Cohort StudiesDokument32 SeitenIntroduction To Epidemiology: Cohort Studiesv_ratNoch keine Bewertungen
- Logistics Management Information Systems (LMIS)Dokument25 SeitenLogistics Management Information Systems (LMIS)v_ratNoch keine Bewertungen
- Day 1 - Equipment-Mohan-1Dokument22 SeitenDay 1 - Equipment-Mohan-1v_ratNoch keine Bewertungen
- Day 4 - CQI in Stores ManagementDokument8 SeitenDay 4 - CQI in Stores Managementv_ratNoch keine Bewertungen
- The Case-Study Approach: Lucy GilsonDokument74 SeitenThe Case-Study Approach: Lucy Gilsonv_ratNoch keine Bewertungen
- Assessment of Patient Engagement With A Mobile Application Among Service Members in TransitionDokument9 SeitenAssessment of Patient Engagement With A Mobile Application Among Service Members in Transitionv_ratNoch keine Bewertungen
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDokument9 SeitenHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To Subscribev_ratNoch keine Bewertungen
- Patient Engagement in Research: A Systematic Review: Researcharticle Open AccessDokument9 SeitenPatient Engagement in Research: A Systematic Review: Researcharticle Open Accessv_ratNoch keine Bewertungen
- Patient Engagement Planning Checklist: Planning Component Key Questions To ConsiderDokument2 SeitenPatient Engagement Planning Checklist: Planning Component Key Questions To Considerv_ratNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Autodesk Nastran In-CAD PDFDokument43 SeitenAutodesk Nastran In-CAD PDFFernando0% (1)
- Caso Estudio: Reliability Analysis of Power Distribution System. A Case StudyDokument6 SeitenCaso Estudio: Reliability Analysis of Power Distribution System. A Case StudyCarlos HernandezNoch keine Bewertungen
- K MCQsDokument6 SeitenK MCQsF ParikhNoch keine Bewertungen
- Physico-Chemical Properties of Nutmeg (Myristica Fragrans Houtt) of North Sulawesi NutmegDokument9 SeitenPhysico-Chemical Properties of Nutmeg (Myristica Fragrans Houtt) of North Sulawesi NutmegZyuha AiniiNoch keine Bewertungen
- ProbDokument10 SeitenProbKashif JawaidNoch keine Bewertungen
- 1st Problem Solving Assignment - Barrels of Apples - M383 Sp22.docx-2Dokument4 Seiten1st Problem Solving Assignment - Barrels of Apples - M383 Sp22.docx-2Kor16Noch keine Bewertungen
- Risk Analysis and Assessment Methodologies in Work SitesDokument49 SeitenRisk Analysis and Assessment Methodologies in Work SitesNhut NguyenNoch keine Bewertungen
- ICU General Admission Orders: OthersDokument2 SeitenICU General Admission Orders: OthersHANIMNoch keine Bewertungen
- What Are The Advantages and Disadvantages of UsingDokument4 SeitenWhat Are The Advantages and Disadvantages of UsingJofet Mendiola88% (8)
- List of HTML TagsDokument5 SeitenList of HTML TagsdorinadidNoch keine Bewertungen
- What Is Denim? Why It's Called Denim?: Properties of Denim FabricDokument21 SeitenWhat Is Denim? Why It's Called Denim?: Properties of Denim Fabricrahmanshanto623100% (1)
- Paper II - Guidelines On The Use of DuctlessDokument51 SeitenPaper II - Guidelines On The Use of DuctlessMohd Khairul Md DinNoch keine Bewertungen
- Electromagnetism WorksheetDokument3 SeitenElectromagnetism WorksheetGuan Jie KhooNoch keine Bewertungen
- BSDDokument26 SeitenBSDEunnicePanaliganNoch keine Bewertungen
- Advanced Physiotherapeutic SyllabusDokument1 SeiteAdvanced Physiotherapeutic SyllabusAnup SharmaNoch keine Bewertungen
- Fluoride - Wide Range of Serious Health Problems"Dokument29 SeitenFluoride - Wide Range of Serious Health Problems"zataullah100% (2)
- Reference by John BatchelorDokument1 SeiteReference by John Batchelorapi-276994844Noch keine Bewertungen
- ASHRAE Elearning Course List - Order FormDokument4 SeitenASHRAE Elearning Course List - Order Formsaquib715Noch keine Bewertungen
- The Serious Student of HistoryDokument5 SeitenThe Serious Student of HistoryCrisanto King CortezNoch keine Bewertungen
- Cpar ReviewerDokument6 SeitenCpar ReviewerHana YeppeodaNoch keine Bewertungen
- Evolis SDK Use Latest IomemDokument10 SeitenEvolis SDK Use Latest IomempatrickNoch keine Bewertungen
- Rab Sikda Optima 2016Dokument20 SeitenRab Sikda Optima 2016Julius Chatry UniwalyNoch keine Bewertungen
- Remedy MidTier Guide 7-5Dokument170 SeitenRemedy MidTier Guide 7-5martin_wiedmeyerNoch keine Bewertungen
- PronounsDokument6 SeitenPronounsHải Dương LêNoch keine Bewertungen
- Trading Journal TDA Branded.v3.5 - W - Total - Transaction - Cost - BlankDokument49 SeitenTrading Journal TDA Branded.v3.5 - W - Total - Transaction - Cost - BlankChristyann LojaNoch keine Bewertungen
- Principles To Action (Short)Dokument6 SeitenPrinciples To Action (Short)nsadie34276Noch keine Bewertungen
- 3g Node B On Ip MediaDokument79 Seiten3g Node B On Ip MediaBsskkd KkdNoch keine Bewertungen
- Aspek Perpajakan Dalam Transfer Pricing: Related PapersDokument15 SeitenAspek Perpajakan Dalam Transfer Pricing: Related PapersHasrawati AzisNoch keine Bewertungen
- Lakh Only) Being The Amount Covered Under The Aforesaid Dishonoured Cheque, and So AlsoDokument2 SeitenLakh Only) Being The Amount Covered Under The Aforesaid Dishonoured Cheque, and So AlsoShivam MishraNoch keine Bewertungen
- KiSoft Sort & Pack Work Station (User Manual)Dokument41 SeitenKiSoft Sort & Pack Work Station (User Manual)Matthew RookeNoch keine Bewertungen