Das könnte Ihnen auch gefallen
- Gale Researcher Guide for: Anxiety and Stress Disorders and PsychiatryVon EverandGale Researcher Guide for: Anxiety and Stress Disorders and PsychiatryNoch keine Bewertungen
- Foa - Kozak 1986 - OPTIONALDokument16 SeitenFoa - Kozak 1986 - OPTIONALCarla MariaNoch keine Bewertungen
- Bye Bye Anxiety and Panic Attacks: Comprehensive CBT guide with techniques and exercises to identify triggers and develop long-term management strategiesVon EverandBye Bye Anxiety and Panic Attacks: Comprehensive CBT guide with techniques and exercises to identify triggers and develop long-term management strategiesNoch keine Bewertungen
- Emotional Processing of Fear. Exposure To Corrective InformationDokument18 SeitenEmotional Processing of Fear. Exposure To Corrective InformationLVNoch keine Bewertungen
- Metacognitive Therapy Hjemdal 2013Dokument13 SeitenMetacognitive Therapy Hjemdal 2013rnuevo2Noch keine Bewertungen
- Barry 2015Dokument15 SeitenBarry 2015José VegaNoch keine Bewertungen
- Introducing Compassion Focused TherapyDokument10 SeitenIntroducing Compassion Focused Therapylwfaxscribd100% (3)
- Systemic Family TherapyDokument19 SeitenSystemic Family TherapyDiego Rojas TorricoNoch keine Bewertungen
- Threat-Related Attentional Bias in Anxious and Nonanxious Individuals: A Meta-Analytic StudyDokument24 SeitenThreat-Related Attentional Bias in Anxious and Nonanxious Individuals: A Meta-Analytic StudySara HeNoch keine Bewertungen
- Article AddictionDokument18 SeitenArticle AddictionAna GazashviliNoch keine Bewertungen
- Cognitive-Behavioral Theory: A. Antonio González-Prendes and Stella M. ReskoDokument27 SeitenCognitive-Behavioral Theory: A. Antonio González-Prendes and Stella M. ReskoRaluca DrbNoch keine Bewertungen
- Beyond The "Psychological Placebo": Specifying The Nonspecific in Psychotherapy (Bjornsson, 2011)Dokument6 SeitenBeyond The "Psychological Placebo": Specifying The Nonspecific in Psychotherapy (Bjornsson, 2011)GokushimakNoch keine Bewertungen
- Brosschot2006 - Emotii Si StresDokument12 SeitenBrosschot2006 - Emotii Si StresgicutaNoch keine Bewertungen
- Ruiz 2014Dokument9 SeitenRuiz 2014ifclarinNoch keine Bewertungen
- Treatment of Complex Posttraumatic SelfDokument11 SeitenTreatment of Complex Posttraumatic Selfcarlo100% (1)
- Motivationasa Mediating Variablebetween Parental Supportand AnxietypublishedDokument20 SeitenMotivationasa Mediating Variablebetween Parental Supportand AnxietypublishedKrizzia Louise B. CabreraNoch keine Bewertungen
- Trauma y Memoria Procedural 2015 Paper Peter LevineDokument18 SeitenTrauma y Memoria Procedural 2015 Paper Peter LevineMaría Regina Castro CataldiNoch keine Bewertungen
- SE Informed Group Psychotherapy For Intl Journal of Group PsychotherapyDokument13 SeitenSE Informed Group Psychotherapy For Intl Journal of Group PsychotherapyLella Misikir100% (1)
- Meditation, Trauma and Suffering in SilenceDokument33 SeitenMeditation, Trauma and Suffering in SilenceIleana Fasick FumeroNoch keine Bewertungen
- ADynamic MaturationalModelANZJFTCrittendenDokument12 SeitenADynamic MaturationalModelANZJFTCrittendenMinh DangNoch keine Bewertungen
- Anxiety-Control Strategies Is There Room For Neutralization in Successful Exposure TreatmentDokument46 SeitenAnxiety-Control Strategies Is There Room For Neutralization in Successful Exposure TreatmentHAnaRoxanaNoch keine Bewertungen
- Mindfulness and Acceptance-Based Behavioral Therapies For Anxiety DisordersDokument13 SeitenMindfulness and Acceptance-Based Behavioral Therapies For Anxiety DisordersAida Esther Hernández SaguarNoch keine Bewertungen
- Practical 1 Maq Kaashvi DubeyDokument23 SeitenPractical 1 Maq Kaashvi Dubeykaashvi dubeyNoch keine Bewertungen
- Craske, Treanor Et Al. 2014Dokument14 SeitenCraske, Treanor Et Al. 2014John NathanNoch keine Bewertungen
- Specificity of Cognitive Emotion Regulation Strategies: A Transdiagnostic ExaminationDokument12 SeitenSpecificity of Cognitive Emotion Regulation Strategies: A Transdiagnostic ExaminationEliana HerediaNoch keine Bewertungen
- Attachment and AnxietyDokument7 SeitenAttachment and Anxietycansu coskunsuNoch keine Bewertungen
- The Six Cycles Maintenance Model Growing A Vicious Flower For DepressionDokument12 SeitenThe Six Cycles Maintenance Model Growing A Vicious Flower For DepressionDIANA SPRINCEANUNoch keine Bewertungen
- Prolonged Exposure Therapy - Past, Present, and FutureDokument5 SeitenProlonged Exposure Therapy - Past, Present, and FutureKelly GCNoch keine Bewertungen
- Anxietysenstivity Er JADDokument12 SeitenAnxietysenstivity Er JADAnonymous YkDJkSqNoch keine Bewertungen
- Foa & Kozak 1986Dokument16 SeitenFoa & Kozak 1986Nim RodNoch keine Bewertungen
- Experiment 4Dokument4 SeitenExperiment 4NiharikaNoch keine Bewertungen
- Anxiety Therapy: Types, Techniques and Worksheets: Heather Lonczak 0 18-02-2020Dokument19 SeitenAnxiety Therapy: Types, Techniques and Worksheets: Heather Lonczak 0 18-02-2020Nadeem Iqbal100% (1)
- The Prefrontal Cortex, Pathological Anxiety, and Anxiety DisordersDokument16 SeitenThe Prefrontal Cortex, Pathological Anxiety, and Anxiety DisordersGabriel Dos SantosNoch keine Bewertungen
- Bork Ovec 2004Dokument31 SeitenBork Ovec 2004Dimitris CharbilasNoch keine Bewertungen
- Aldao20Nolen Hoeksema20201020ER20strategies20transdiagnostic20BRATDokument11 SeitenAldao20Nolen Hoeksema20201020ER20strategies20transdiagnostic20BRATAlejandra BilbaoNoch keine Bewertungen
- McEvoy 2019 Review MCT Anxiety DisordersDokument9 SeitenMcEvoy 2019 Review MCT Anxiety DisordersmarggiNoch keine Bewertungen
- Roussis & Wells, 2006Dokument12 SeitenRoussis & Wells, 2006Arckantos26Noch keine Bewertungen
- PTSD Articol ȘtiințificDokument14 SeitenPTSD Articol ȘtiințificValentinaNoch keine Bewertungen
- IntroducingCompassionFocusedTherapy (Gilbert, 2009)Dokument10 SeitenIntroducingCompassionFocusedTherapy (Gilbert, 2009)MiguelySusy Ramos-RojasNoch keine Bewertungen
- The Place of The Unconscious in Mental Health Nursing: Eature RticleDokument7 SeitenThe Place of The Unconscious in Mental Health Nursing: Eature Rticlehana tashyaNoch keine Bewertungen
- Functional and Dysfunctional Aspects of Social AnxietyDokument32 SeitenFunctional and Dysfunctional Aspects of Social Anxietymuiescr1bdNoch keine Bewertungen
- Neuroanatomia Funcional Machado 3 Ed 2014Dokument34 SeitenNeuroanatomia Funcional Machado 3 Ed 2014ThiagoSoaresNoch keine Bewertungen
- TheoreticalDokument5 SeitenTheoreticallexschub12Noch keine Bewertungen
- 1743 Using Compassion Focused Therapy To Work With Shame and Self Criticism in Complex TraumaDokument8 Seiten1743 Using Compassion Focused Therapy To Work With Shame and Self Criticism in Complex TraumaA Zakiy MohsinNoch keine Bewertungen
- Clinical Assessment of Psychological Adaptive Mechanisms in Medical SettingsDokument13 SeitenClinical Assessment of Psychological Adaptive Mechanisms in Medical SettingsAdrian GuzmanNoch keine Bewertungen
- Haunted SelfDokument2 SeitenHaunted SelfCellaNoch keine Bewertungen
- Treatment of Anxious Attachment in Infancy and Early ChildhoodDokument67 SeitenTreatment of Anxious Attachment in Infancy and Early ChildhoodFernando Hilario VillapecellínNoch keine Bewertungen
- Humanism As A Common Factor in PsychotherapyDokument6 SeitenHumanism As A Common Factor in PsychotherapyMaRice Mar RiceNoch keine Bewertungen
- Leahy - Emotional Schemas and Self-HelpDokument6 SeitenLeahy - Emotional Schemas and Self-HelpLívia Frias100% (1)
- Introducing Compassion-Focused Therapy-Gilbert PDFDokument10 SeitenIntroducing Compassion-Focused Therapy-Gilbert PDFThomas KilroyNoch keine Bewertungen
- MEtacognitive Approach History and Third WaveDokument10 SeitenMEtacognitive Approach History and Third WaveGuido WoWNoch keine Bewertungen
- Neuroscience and Biobehavioral Reviews: A B 1 A C 1 DDokument9 SeitenNeuroscience and Biobehavioral Reviews: A B 1 A C 1 DMeilisa KusdiantoNoch keine Bewertungen
- AnxietyDokument24 SeitenAnxietyPedro Luis Martinez SanjuanNoch keine Bewertungen
- Transformative Processes in Psychotherapy: How Patients Work in Therapy To Overcome Their ProblemsDokument6 SeitenTransformative Processes in Psychotherapy: How Patients Work in Therapy To Overcome Their ProblemsChong Hiu Pun100% (1)
- Chapter 19. Fear and Anxiety2Dokument17 SeitenChapter 19. Fear and Anxiety2Costrut LaurNoch keine Bewertungen
- AnxietyDokument15 SeitenAnxietydfre345100% (1)
- Borderline Si Psihoterapia SistemicaDokument19 SeitenBorderline Si Psihoterapia Sistemicaa.vieru96Noch keine Bewertungen
- Evolucion de La Depresion, Cuestiones y ImplicacionesDokument11 SeitenEvolucion de La Depresion, Cuestiones y ImplicacionesIVAN DARIO RODRIGUEZ SALAMANCANoch keine Bewertungen
- Coping: Strategies: Problem SolvingDokument12 SeitenCoping: Strategies: Problem SolvingNidhi DNoch keine Bewertungen
- Wright 2009Dokument13 SeitenWright 20092332801101Noch keine Bewertungen
- Gilbert KeynoteDokument14 SeitenGilbert KeynoteShandy PutraNoch keine Bewertungen
- Developing Self Compassion As A Resource For Coping With Hardship: Exploring The Potential of Compassion Focused TherapyDokument14 SeitenDeveloping Self Compassion As A Resource For Coping With Hardship: Exploring The Potential of Compassion Focused TherapyShandy PutraNoch keine Bewertungen
- Psychotherapeutic Bene Fits of Compassion-Focused Therapy: An Early Systematic ReviewDokument19 SeitenPsychotherapeutic Bene Fits of Compassion-Focused Therapy: An Early Systematic ReviewShandy PutraNoch keine Bewertungen
- Kirby 2017Dokument25 SeitenKirby 2017Shandy PutraNoch keine Bewertungen
- Temel Atalay2018Dokument8 SeitenTemel Atalay2018Esther DanNoch keine Bewertungen
- The Effectiveness of Compassion-Focused Therapy On The Infertile Women DepressionDokument14 SeitenThe Effectiveness of Compassion-Focused Therapy On The Infertile Women DepressionShandy PutraNoch keine Bewertungen
- Sacristan-Martin Et Al - Trials Nov 2019Dokument15 SeitenSacristan-Martin Et Al - Trials Nov 2019olgasacristan316Noch keine Bewertungen
- 9780415448079Dokument13 Seiten9780415448079Shandy PutraNoch keine Bewertungen
- Compassionate Mind TrainingDokument28 SeitenCompassionate Mind TrainingSoulyoga100% (1)
- Adult HmpanicDokument9 SeitenAdult HmpanicShandy PutraNoch keine Bewertungen
- Practicing Self-Compassion Weakens The Relationship Between Fear of Receiving Compassion and The Desire To Conceal Negative Experiences From OthersDokument12 SeitenPracticing Self-Compassion Weakens The Relationship Between Fear of Receiving Compassion and The Desire To Conceal Negative Experiences From OthersShandy PutraNoch keine Bewertungen
- Child Abuse & Neglect: Full Length ArticleDokument9 SeitenChild Abuse & Neglect: Full Length ArticleShandy PutraNoch keine Bewertungen
- Patofis Delusion PDFDokument12 SeitenPatofis Delusion PDFStephen NathanielNoch keine Bewertungen
- Akiskal 1983Dokument10 SeitenAkiskal 1983Shandy PutraNoch keine Bewertungen
- To Believe or Not To Believe Cognitive and Psychod PDFDokument12 SeitenTo Believe or Not To Believe Cognitive and Psychod PDFShandy PutraNoch keine Bewertungen
- Psychologicaltheoriesofdelusionaldisorder 170623003843Dokument30 SeitenPsychologicaltheoriesofdelusionaldisorder 170623003843Shandy PutraNoch keine Bewertungen
- Ventimiglia 2018Dokument14 SeitenVentimiglia 2018Shandy PutraNoch keine Bewertungen
- Reaksi Skizofrenia, Depresi Dan ManicDokument23 SeitenReaksi Skizofrenia, Depresi Dan ManicShandy PutraNoch keine Bewertungen
- CBTP Modul 6 For VoicesDokument6 SeitenCBTP Modul 6 For VoicesShandy PutraNoch keine Bewertungen
- Understanding DelusionsDokument35 SeitenUnderstanding DelusionsShandy PutraNoch keine Bewertungen
- Persistent Delusional DisorderDokument4 SeitenPersistent Delusional DisorderShandy PutraNoch keine Bewertungen
- To Believe or Not To Believe Cognitive and Psychod PDFDokument12 SeitenTo Believe or Not To Believe Cognitive and Psychod PDFShandy PutraNoch keine Bewertungen
- Peer Support DefinedDokument11 SeitenPeer Support DefinedShandy PutraNoch keine Bewertungen
- 11-Rubber & PlasticsDokument48 Seiten11-Rubber & PlasticsJack NgNoch keine Bewertungen
- Poster-Shading PaperDokument1 SeitePoster-Shading PaperOsama AljenabiNoch keine Bewertungen
- TPDokument10 SeitenTPfaisal gaziNoch keine Bewertungen
- Misc 8DNL 8MPL 8MPN B PDFDokument41 SeitenMisc 8DNL 8MPL 8MPN B PDFVesica PiscesNoch keine Bewertungen
- KK AggarwalDokument412 SeitenKK AggarwalEnrico Miguel AquinoNoch keine Bewertungen
- Nominal GroupDokument3 SeitenNominal GroupSrourNoch keine Bewertungen
- Internal Resistance To Corrosion in SHS - To Go On WebsiteDokument48 SeitenInternal Resistance To Corrosion in SHS - To Go On WebsitetheodorebayuNoch keine Bewertungen
- Chapter 01 What Is Statistics?Dokument18 SeitenChapter 01 What Is Statistics?windyuriNoch keine Bewertungen
- Calculating Free Energies Using Adaptive Biasing Force MethodDokument14 SeitenCalculating Free Energies Using Adaptive Biasing Force MethodAmin SagarNoch keine Bewertungen
- AP8 Q4 Ip9 V.02Dokument7 SeitenAP8 Q4 Ip9 V.02nikka suitadoNoch keine Bewertungen
- Bone Surface MarkingsDokument2 SeitenBone Surface MarkingsNurul Afiqah Fattin AmatNoch keine Bewertungen
- Aristotle - OCR - AS Revision NotesDokument3 SeitenAristotle - OCR - AS Revision NotesAmelia Dovelle0% (1)
- Maximum and Minimum PDFDokument3 SeitenMaximum and Minimum PDFChai Usajai UsajaiNoch keine Bewertungen
- Saflex-Dg - 41 Data SheetDokument5 SeitenSaflex-Dg - 41 Data SheetrasheedgotzNoch keine Bewertungen
- Life and Works of Jose Rizal Modified ModuleDokument96 SeitenLife and Works of Jose Rizal Modified ModuleRamos, Queencie R.Noch keine Bewertungen
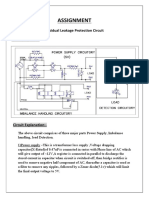
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDokument2 SeitenAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNoch keine Bewertungen
- Audi A4-7Dokument532 SeitenAudi A4-7Anonymous QRVqOsa5Noch keine Bewertungen
- Digital Systems Project: IITB CPUDokument7 SeitenDigital Systems Project: IITB CPUAnoushka DeyNoch keine Bewertungen
- I. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)Dokument5 SeitenI. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)thmeiz.17sNoch keine Bewertungen
- Taylor Series PDFDokument147 SeitenTaylor Series PDFDean HaynesNoch keine Bewertungen
- 12 Step Worksheet With QuestionsDokument26 Seiten12 Step Worksheet With QuestionsKristinDaigleNoch keine Bewertungen
- Leveriza Heights SubdivisionDokument4 SeitenLeveriza Heights SubdivisionTabordan AlmaeNoch keine Bewertungen
- FT2020Dokument7 SeitenFT2020Sam SparksNoch keine Bewertungen
- Dog & Kitten: XshaperDokument17 SeitenDog & Kitten: XshaperAll PrintNoch keine Bewertungen
- FINAL SMAC Compressor Control Philosophy Rev4Dokument6 SeitenFINAL SMAC Compressor Control Philosophy Rev4AhmedNoch keine Bewertungen
- JUnit 5 User GuideDokument90 SeitenJUnit 5 User GuideaawaakNoch keine Bewertungen
- CM2192 - High Performance Liquid Chromatography For Rapid Separation and Analysis of A Vitamin C TabletDokument2 SeitenCM2192 - High Performance Liquid Chromatography For Rapid Separation and Analysis of A Vitamin C TabletJames HookNoch keine Bewertungen
- Darkle Slideshow by SlidesgoDokument53 SeitenDarkle Slideshow by SlidesgoADITI GUPTANoch keine Bewertungen
- Topic: Grammatical Issues: What Are Parts of Speech?Dokument122 SeitenTopic: Grammatical Issues: What Are Parts of Speech?AK AKASHNoch keine Bewertungen
- Class 12 Physics Derivations Shobhit NirwanDokument6 SeitenClass 12 Physics Derivations Shobhit Nirwanaastha.sawlaniNoch keine Bewertungen
- An Autobiography of Trauma: A Healing JourneyVon EverandAn Autobiography of Trauma: A Healing JourneyBewertung: 5 von 5 Sternen5/5 (2)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesVon EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesBewertung: 5 von 5 Sternen5/5 (70)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryVon EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryBewertung: 4.5 von 5 Sternen4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreVon EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreBewertung: 5 von 5 Sternen5/5 (17)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionVon EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNoch keine Bewertungen
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeVon EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeBewertung: 4.5 von 5 Sternen4.5/5 (140)
- Don't Panic: Taking Control of Anxiety AttacksVon EverandDon't Panic: Taking Control of Anxiety AttacksBewertung: 4 von 5 Sternen4/5 (12)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeVon EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeBewertung: 4.5 von 5 Sternen4.5/5 (49)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationVon EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationBewertung: 5 von 5 Sternen5/5 (9)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDVon EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDBewertung: 4.5 von 5 Sternen4.5/5 (167)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisVon EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisBewertung: 5 von 5 Sternen5/5 (5)
- Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensVon EverandBrain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensBewertung: 5 von 5 Sternen5/5 (2)
- Triggers: How We Can Stop Reacting and Start HealingVon EverandTriggers: How We Can Stop Reacting and Start HealingBewertung: 5 von 5 Sternen5/5 (58)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaVon EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaBewertung: 4.5 von 5 Sternen4.5/5 (56)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeVon EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeBewertung: 5 von 5 Sternen5/5 (558)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackVon EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackBewertung: 4.5 von 5 Sternen4.5/5 (152)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONVon EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONBewertung: 4.5 von 5 Sternen4.5/5 (24)
- I Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionVon EverandI Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionBewertung: 4.5 von 5 Sternen4.5/5 (106)
- Anxious for Nothing: Finding Calm in a Chaotic WorldVon EverandAnxious for Nothing: Finding Calm in a Chaotic WorldBewertung: 4.5 von 5 Sternen4.5/5 (1245)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentVon EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNoch keine Bewertungen
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItVon EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItBewertung: 4.5 von 5 Sternen4.5/5 (107)