Das könnte Ihnen auch gefallen
- PALS Precourse Self-AssessmentDokument2 SeitenPALS Precourse Self-AssessmentGabriel Del RosarioNoch keine Bewertungen
- EDHKL ACLS Manual - Final Edit (1) - 1Dokument43 SeitenEDHKL ACLS Manual - Final Edit (1) - 1Nurhafizah IbrahimNoch keine Bewertungen
- PALS Precourse Self-Assessment RiaDokument3 SeitenPALS Precourse Self-Assessment RiaAde Novian ParmudityaNoch keine Bewertungen
- American Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityDokument49 SeitenAmerican Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityZulkarnainBustamamNoch keine Bewertungen
- 2020 Acls Megacode Testing Scenarios - 2Dokument13 Seiten2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNoch keine Bewertungen
- Megacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...Dokument1 SeiteMegacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...krgduraiNoch keine Bewertungen
- ACLS Protocols Pocket VersionDokument2 SeitenACLS Protocols Pocket Versionjohndoe1995Noch keine Bewertungen
- BLS SummaryDokument2 SeitenBLS Summaryreyes markNoch keine Bewertungen
- Pals Coaching Center in HyderabadDokument3 SeitenPals Coaching Center in HyderabadcardiaceduNoch keine Bewertungen
- Basic Life Support (BLS) Training Course: FeaturesDokument1 SeiteBasic Life Support (BLS) Training Course: FeaturesSheryl Fuentes De GuzmanNoch keine Bewertungen
- Advanced Paediatric Life Support - A0 PDFDokument1 SeiteAdvanced Paediatric Life Support - A0 PDFiulia-uroNoch keine Bewertungen
- Antrim ED Handbook 2019Dokument238 SeitenAntrim ED Handbook 2019Chris Jardine LiNoch keine Bewertungen
- Ottawas Clerkship GuideDokument44 SeitenOttawas Clerkship GuideHugo LuceroNoch keine Bewertungen
- Pepp Als PretestDokument4 SeitenPepp Als PretestDave BoppNoch keine Bewertungen
- Acls AnpDokument20 SeitenAcls AnpNirupama KsNoch keine Bewertungen
- 2011 BLS HCP Exam BinderDokument24 Seiten2011 BLS HCP Exam Bindermag griffNoch keine Bewertungen
- Advanced Trauma Life Support RevisedDokument7 SeitenAdvanced Trauma Life Support RevisedpaveethrahNoch keine Bewertungen
- AHA ACLS Written Test: Ready To Study? Start With FlashcardsDokument8 SeitenAHA ACLS Written Test: Ready To Study? Start With FlashcardssallyNoch keine Bewertungen
- ACLS ScenarioDokument21 SeitenACLS Scenariomarves15Noch keine Bewertungen
- Trauma and Shock ATLSDokument19 SeitenTrauma and Shock ATLSDrChauhan100% (2)
- Guidelines Adult Advanced Life SupportDokument35 SeitenGuidelines Adult Advanced Life SupportindahNoch keine Bewertungen
- BLS & AclsDokument29 SeitenBLS & AclswcgokulNoch keine Bewertungen
- PEARS Handout 2016Dokument8 SeitenPEARS Handout 2016Carrie DAndreaNoch keine Bewertungen
- Paediatric ECG Checklist 3.8Dokument2 SeitenPaediatric ECG Checklist 3.8Muhammad Moazzam GulzarNoch keine Bewertungen
- 3 Minute EM Student PresentationDokument5 Seiten3 Minute EM Student Presentationdebra_euromNoch keine Bewertungen
- Advanced Cardiovascular Life Support (ACLS)Dokument2 SeitenAdvanced Cardiovascular Life Support (ACLS)Vijay MgNoch keine Bewertungen
- PICU Common ProblemDokument49 SeitenPICU Common ProblemRawabi rawabi1997Noch keine Bewertungen
- ACLS Training - Most Important Points To RememberDokument5 SeitenACLS Training - Most Important Points To RememberEman ElzeftawyNoch keine Bewertungen
- Acls Review 2015Dokument29 SeitenAcls Review 2015JB Reyes100% (2)
- AHA PALS Core Case Test ChecklistsDokument12 SeitenAHA PALS Core Case Test ChecklistsVitor Hugo G CorreiaNoch keine Bewertungen
- BLS Skills Session Checklist and Test CompleteDokument14 SeitenBLS Skills Session Checklist and Test Completeicups baptisbatuNoch keine Bewertungen
- Obert GagnéDokument5 SeitenObert GagnéKamalz JuniorNoch keine Bewertungen
- ATLS-9e Trauma Flow Sheet PDFDokument4 SeitenATLS-9e Trauma Flow Sheet PDFWaeel HamoudaNoch keine Bewertungen
- Normal Ranges Vital Signs 2017Dokument2 SeitenNormal Ranges Vital Signs 2017Elvis Nguyen100% (1)
- BLS FinalDokument47 SeitenBLS Finalshouvik chowdhury100% (1)
- ACLS Simulation ScenariosDokument14 SeitenACLS Simulation ScenariosVanessa HermioneNoch keine Bewertungen
- EKG - Basic Interpretation and ACLS PreparationDokument39 SeitenEKG - Basic Interpretation and ACLS PreparationSergio Cano100% (2)
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDokument1 SeiteAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNoch keine Bewertungen
- Algorithm-ACLS CA in Pregnancy In-Hospital 200612Dokument1 SeiteAlgorithm-ACLS CA in Pregnancy In-Hospital 200612Hyunsoo EllisNoch keine Bewertungen
- Paediatric Advanced Life Support: Resuscitation Council (UK)Dokument12 SeitenPaediatric Advanced Life Support: Resuscitation Council (UK)zacklim_2000100% (1)
- DIT High Yield Questions PDFDokument13 SeitenDIT High Yield Questions PDFjoshNoch keine Bewertungen
- Approach To TruamaDokument29 SeitenApproach To TruamaIbsa ShumaNoch keine Bewertungen
- Faculty Guide For ACLS Instructor Course (PDF Library)Dokument58 SeitenFaculty Guide For ACLS Instructor Course (PDF Library)Ogine L. LoNoch keine Bewertungen
- STEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3Dokument39 SeitenSTEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3elesia powell100% (1)
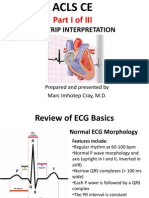
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalDokument80 SeitenACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- Paediatric Advanced Life Support GuidelinesDokument31 SeitenPaediatric Advanced Life Support GuidelinesEXODUSGENNoch keine Bewertungen
- Acls DrugsDokument5 SeitenAcls DrugsDebby Christiana SNoch keine Bewertungen
- AHA InstructorDokument7 SeitenAHA InstructorBinoy GopinathanNoch keine Bewertungen
- CPR ACLS Study GuideDokument18 SeitenCPR ACLS Study GuideJohn Phamacy100% (1)
- ToxidromesDokument1 SeiteToxidromesMayer Rosenberg100% (7)
- ACLS NotesDokument3 SeitenACLS Notessaxmanwrv0% (1)
- Pals Study GuideDokument8 SeitenPals Study Guidefredyromanreyes100% (2)
- Critical Care SedationVon EverandCritical Care SedationAngelo Raffaele De GaudioNoch keine Bewertungen
- Basic ECGDokument152 SeitenBasic ECGTuấn Thanh VõNoch keine Bewertungen
- Hypoxemic Resp. FailureDokument52 SeitenHypoxemic Resp. FailureLovely Acabado TampocoNoch keine Bewertungen
- I.C.U. Chest Radiology: Principles and Case StudiesVon EverandI.C.U. Chest Radiology: Principles and Case StudiesNoch keine Bewertungen
- Estimate LEL and FlashDokument2 SeitenEstimate LEL and Flashnirmal_subudhiNoch keine Bewertungen
- RM50HG 12SDokument3 SeitenRM50HG 12SAbu Bakr M. SaeedNoch keine Bewertungen
- CHAPTER 7 Project Management and Network AnalysisDokument31 SeitenCHAPTER 7 Project Management and Network AnalysisNitinNoch keine Bewertungen
- 12 Pipes and CisternDokument40 Seiten12 Pipes and Cisternhemanth kumarNoch keine Bewertungen
- Year 8 Mid-Term Maths TestDokument7 SeitenYear 8 Mid-Term Maths TestJenniferNoch keine Bewertungen
- Working Paper 2010Dokument76 SeitenWorking Paper 2010Javed LatifNoch keine Bewertungen
- Agricultural Crop ProductionDokument10 SeitenAgricultural Crop ProductionElisha Liwag100% (1)
- Experiment 4 Determination of Total Hardness As PPM Calcium CarbonateDokument26 SeitenExperiment 4 Determination of Total Hardness As PPM Calcium CarbonateJordanNoch keine Bewertungen
- Issa Components of Tactical ConditioningDokument37 SeitenIssa Components of Tactical Conditioningamirreza jm100% (2)
- MSDS Black Magic Shampoo 03.21.12Dokument5 SeitenMSDS Black Magic Shampoo 03.21.12Pure PawsNoch keine Bewertungen
- Emmvee Solarizer Elite Hybrid BrochureDokument4 SeitenEmmvee Solarizer Elite Hybrid BrochurePushkraj PatilNoch keine Bewertungen
- Tjo 35 2 139Dokument11 SeitenTjo 35 2 139Manuel CastilloNoch keine Bewertungen
- Green Line UndergroundDokument2 SeitenGreen Line UndergroundFrancisco M. RamosNoch keine Bewertungen
- 8051 Interfacing With Display SevicesDokument5 Seiten8051 Interfacing With Display Sevicesramjee26100% (1)
- L3 Role of EHO and AEHO in MalaysiaDokument37 SeitenL3 Role of EHO and AEHO in MalaysiaNandakumaran SelvakumaranNoch keine Bewertungen
- Worksheet Unit 1 Health Problems 6th Grade 2022Dokument8 SeitenWorksheet Unit 1 Health Problems 6th Grade 2022amandaNoch keine Bewertungen
- 2.4 The Surge Protection Device (SPD) : PrincipleDokument1 Seite2.4 The Surge Protection Device (SPD) : Principlemahmoud12122012Noch keine Bewertungen
- Asdadfwassfbdfbdsbfdfsb PDFDokument6 SeitenAsdadfwassfbdfbdsbfdfsb PDFpNoch keine Bewertungen
- Glycosides: Prepared by Asma ManzoorDokument94 SeitenGlycosides: Prepared by Asma ManzoorAsma khanNoch keine Bewertungen
- The Aeroponic SystemDokument15 SeitenThe Aeroponic SystemLiviu AngelescuNoch keine Bewertungen
- 09 - Carbon Dioxide - G71143R04Dokument5 Seiten09 - Carbon Dioxide - G71143R04chem.rajavithiNoch keine Bewertungen
- Attack On The Pratzeberg: French ForcesDokument3 SeitenAttack On The Pratzeberg: French ForceswimNoch keine Bewertungen
- A3233q48 140313 V01 enDokument15 SeitenA3233q48 140313 V01 enfreezsoli4576Noch keine Bewertungen
- Latvian VocabularyDokument6 SeitenLatvian Vocabularyparajms8778Noch keine Bewertungen
- Smart Cities - A Case Study in Waste Monitoring and ManagementDokument10 SeitenSmart Cities - A Case Study in Waste Monitoring and Managementfaris100% (1)
- Autumn The Bear Girl: by JojilieDokument9 SeitenAutumn The Bear Girl: by JojilieBrenda Acuña100% (1)
- Node2vec: Scalable Feature Learning For Networks: Aditya Grover Et Al. Presented By: Saim Mehmood Ahmadreza JeddiDokument30 SeitenNode2vec: Scalable Feature Learning For Networks: Aditya Grover Et Al. Presented By: Saim Mehmood Ahmadreza Jeddisiraj mohammedNoch keine Bewertungen
- Brooklyn Brochure 21aprilDokument14 SeitenBrooklyn Brochure 21aprilRiya AgrawalNoch keine Bewertungen
- The Western Desert Versus Nile Delta A C PDFDokument17 SeitenThe Western Desert Versus Nile Delta A C PDFSohini ChatterjeeNoch keine Bewertungen
- Safety Data Sheet: NEOPOR 2200Dokument11 SeitenSafety Data Sheet: NEOPOR 2200Şerbuţă AlexandruNoch keine Bewertungen