Das könnte Ihnen auch gefallen
- Metformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometDokument5 SeitenMetformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometAgronaSlaughterNoch keine Bewertungen
- AtorvastatinDokument2 SeitenAtorvastatinitsmeaya0% (2)
- SucralfateDokument3 SeitenSucralfateViziteu AlexandraNoch keine Bewertungen
- Drug Study CHDCDokument1 SeiteDrug Study CHDCIannBlancoNoch keine Bewertungen
- Ertapenem (Invanz)Dokument1 SeiteErtapenem (Invanz)Adrianne BazoNoch keine Bewertungen
- Omeprazole, Potassium Chloride, Citicoline, GlimepirideDokument5 SeitenOmeprazole, Potassium Chloride, Citicoline, GlimepirideJenivic Empig PuedanNoch keine Bewertungen
- Drug Study.Dokument9 SeitenDrug Study.Chelsea Therese GuevarraNoch keine Bewertungen
- Tablets: Tablets (Chewable) : Tablets (Extended-Release)Dokument1 SeiteTablets: Tablets (Chewable) : Tablets (Extended-Release)Melissa Marie CustodioNoch keine Bewertungen
- PrednisoneDokument3 SeitenPrednisoneMaja DeraNoch keine Bewertungen
- Pathophysiology of Nephrotic SyndromeDokument1 SeitePathophysiology of Nephrotic SyndromeKristian Karl Bautista Kiw-isNoch keine Bewertungen
- PonstanDokument2 SeitenPonstanianecunar100% (2)
- Frisium Knowledge ModuleDokument7 SeitenFrisium Knowledge ModulesiddiqrehanNoch keine Bewertungen
- Suxamethonium Chloride Injection Bp-PiDokument8 SeitenSuxamethonium Chloride Injection Bp-PinanaNoch keine Bewertungen
- DRUGSDokument5 SeitenDRUGSDanica EspejoNoch keine Bewertungen
- Emergency Drug StudyDokument3 SeitenEmergency Drug StudyGrace Santos MirandaNoch keine Bewertungen
- Cerebral Palsy Discharge PlanningDokument3 SeitenCerebral Palsy Discharge Planningjints poterNoch keine Bewertungen
- Drug Study AzithromycinDokument2 SeitenDrug Study AzithromycinYamete KudasaiNoch keine Bewertungen
- CimetidineDokument3 SeitenCimetidineapi-3797941Noch keine Bewertungen
- Dolan Drug StudyDokument3 SeitenDolan Drug StudyLian Robbie BautistaNoch keine Bewertungen
- Nurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Dokument2 SeitenNurse'Sdrug Handbook Jones & Bartlett Learning 14 Edition 2015Bianca Nicole Gacad FernandezNoch keine Bewertungen
- Drug StudyDokument6 SeitenDrug StudyChickz HunterNoch keine Bewertungen
- Drug Study: Davao Doctors College General Malvar ST., Davao City Nursing ProgramDokument3 SeitenDrug Study: Davao Doctors College General Malvar ST., Davao City Nursing ProgramJear RomeroNoch keine Bewertungen
- Name Mucosta Tablets 100 Description PDFDokument7 SeitenName Mucosta Tablets 100 Description PDFnanda RaharjaNoch keine Bewertungen
- Colchicine FDADokument24 SeitenColchicine FDACatalina BanuNoch keine Bewertungen
- Celecoxib CelebrexDokument1 SeiteCelecoxib CelebrexBeverly Ann de LeonNoch keine Bewertungen
- Torvastatin Drug StudyDokument2 SeitenTorvastatin Drug StudyRoland YusteNoch keine Bewertungen
- Drug StudyDokument3 SeitenDrug StudyMarychen Cabunas100% (1)
- Rathna Drug Card in (Lovenox)Dokument1 SeiteRathna Drug Card in (Lovenox)erdos13Noch keine Bewertungen
- Lived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationDokument20 SeitenLived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationPsychology and Education: A Multidisciplinary JournalNoch keine Bewertungen
- Lui Sh-Colored Lips and Finger Nails Blur Red VisionDokument1 SeiteLui Sh-Colored Lips and Finger Nails Blur Red VisionMagdayao Romamea100% (1)
- KetoconazoleDokument2 SeitenKetoconazoleMD. DELWAR HOSSAINNoch keine Bewertungen
- The Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016Dokument10 SeitenThe Format of This Leaflet Was Determined by The Ministry of Health and Its Content Was Checked and Approved by It On February 2016ddandan_2Noch keine Bewertungen
- Tinidazole Is An AntiDokument6 SeitenTinidazole Is An AntiNoi Maya Anggrita SariNoch keine Bewertungen
- PSYCHIAdrugstudyDokument5 SeitenPSYCHIAdrugstudyJss Rosete-De GuzmanNoch keine Bewertungen
- LAMOTRIGINEDokument2 SeitenLAMOTRIGINEJOHNNoch keine Bewertungen
- MoclodemideDokument1 SeiteMoclodemideArnzz AgbulosNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug StudyGian Era100% (1)
- DRUG StudyDokument6 SeitenDRUG StudyJheryck SabadaoNoch keine Bewertungen
- Tetanus Immune Globulin: Deanzel Jade TrazonaDokument9 SeitenTetanus Immune Globulin: Deanzel Jade TrazonaIrene Grace BalcuevaNoch keine Bewertungen
- Side Effects:: AtropineDokument7 SeitenSide Effects:: AtropinekletadaNoch keine Bewertungen
- Betahistine Drug InfoDokument3 SeitenBetahistine Drug InfoAshish KarnNoch keine Bewertungen
- ER Journal Summary - Effects of An Ethical Empowerment Program On Critical Care Nurses' Ethical Decision-MakingDokument1 SeiteER Journal Summary - Effects of An Ethical Empowerment Program On Critical Care Nurses' Ethical Decision-MakingWyen CabatbatNoch keine Bewertungen
- DrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Dokument2 SeitenDrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Coleen Mae CamaristaNoch keine Bewertungen
- Nifedipine and Prednisone Drug StudyDokument4 SeitenNifedipine and Prednisone Drug StudyJomer GonzalesNoch keine Bewertungen
- © The Mechanism of Action of Anectine Involves What Appears To Be A "Persistent"Dokument6 Seiten© The Mechanism of Action of Anectine Involves What Appears To Be A "Persistent"kaye marie100% (1)
- IFOSFAMIDEDokument4 SeitenIFOSFAMIDEErza GenatrikaNoch keine Bewertungen
- CefadroxilDokument2 SeitenCefadroxilArvie AlvarezNoch keine Bewertungen
- PantoprazoleDokument1 SeitePantoprazolehahahahaaaaaaaNoch keine Bewertungen
- Drug Study KeterolacDokument2 SeitenDrug Study KeterolacKillerBall RegioNoch keine Bewertungen
- Dosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Dokument3 SeitenDosage: 50 MG Order: PRN q6h Route: IV (Case Scenario Based)Edward Luis EsguerraNoch keine Bewertungen
- Drug Study RopivacaineDokument2 SeitenDrug Study Ropivacainerica sebabillonesNoch keine Bewertungen
- Levalbuterol XopenexDokument2 SeitenLevalbuterol XopenexCassie100% (1)
- Drug StudyDokument2 SeitenDrug Studymegreen GamingNoch keine Bewertungen
- Drug Analysis CefoxitinDokument2 SeitenDrug Analysis CefoxitinNika LoNoch keine Bewertungen
- Drug Study: Aspirin (Asa)Dokument5 SeitenDrug Study: Aspirin (Asa)Shara Lailanie A. AzisNoch keine Bewertungen
- Jentadueto 2.5 MG - 1,000 MG (Emc)Dokument20 SeitenJentadueto 2.5 MG - 1,000 MG (Emc)VENKATA RAJA ALURINoch keine Bewertungen
- Cetapin XR Aug 2017 FinalDokument8 SeitenCetapin XR Aug 2017 FinalKaushika KalaiNoch keine Bewertungen
- Metformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetDokument11 SeitenMetformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetAfifa ZainNoch keine Bewertungen
- FR H 6788 001 FinalSPCDokument28 SeitenFR H 6788 001 FinalSPCabenezer g/kirstosNoch keine Bewertungen
- Initial Treatment: Special WarningsDokument10 SeitenInitial Treatment: Special Warningsddandan_2Noch keine Bewertungen
- Summary of Product CharacteristicsDokument24 SeitenSummary of Product Characteristicsddandan_2Noch keine Bewertungen
- Estradiol As Hemihydrate 3.2mg (Evorel - 50)Dokument20 SeitenEstradiol As Hemihydrate 3.2mg (Evorel - 50)ddandan_2Noch keine Bewertungen
- Adapalene 0.1% (Adaferin Cream)Dokument6 SeitenAdapalene 0.1% (Adaferin Cream)ddandan_2Noch keine Bewertungen
- AMARYL 1mg, 2mg, 3mg, 4mg: 1 Indications and UsageDokument16 SeitenAMARYL 1mg, 2mg, 3mg, 4mg: 1 Indications and Usageddandan_2Noch keine Bewertungen
- Haloperidol 2mg-ml DropsDokument15 SeitenHaloperidol 2mg-ml Dropsddandan_2Noch keine Bewertungen
- The Content of This Leaflet Was Updated According To The Guidelines of The Ministry of Health in September 2017Dokument14 SeitenThe Content of This Leaflet Was Updated According To The Guidelines of The Ministry of Health in September 2017ddandan_2Noch keine Bewertungen
- Aclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)Dokument22 SeitenAclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)ddandan_2Noch keine Bewertungen
- BaclofenDokument11 SeitenBaclofenddandan_2Noch keine Bewertungen
- Zofran Tablets 4mg Zofran Tablets 8mg: 1. Trade Name of The Medicinal ProductDokument12 SeitenZofran Tablets 4mg Zofran Tablets 8mg: 1. Trade Name of The Medicinal Productddandan_2Noch keine Bewertungen
- Cataflam: (Diclofenac Potassium)Dokument10 SeitenCataflam: (Diclofenac Potassium)ddandan_2Noch keine Bewertungen
- Summary of Product Characteristics: Edronax 4 MGDokument9 SeitenSummary of Product Characteristics: Edronax 4 MGddandan_2Noch keine Bewertungen
- Levodopa 250mg + Carbidopa 25mg (Dopicar)Dokument10 SeitenLevodopa 250mg + Carbidopa 25mg (Dopicar)ddandan_2Noch keine Bewertungen
- Dekinet Tablets: Use in PregnancyDokument3 SeitenDekinet Tablets: Use in Pregnancyddandan_2Noch keine Bewertungen
- Adapalene 0.1% (Adaferin Gel)Dokument4 SeitenAdapalene 0.1% (Adaferin Gel)ddandan_2Noch keine Bewertungen
- AnastrozoleDokument13 SeitenAnastrozoleddandan_2Noch keine Bewertungen
- Doctor Leaflet: 1. Name of The Medicinal Product: Budeson 3 MGDokument11 SeitenDoctor Leaflet: 1. Name of The Medicinal Product: Budeson 3 MGddandan_2Noch keine Bewertungen
- Netupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)Dokument16 SeitenNetupitant 300mg + Palonosetron HCL 0.56mg (Akynzeo)ddandan_2Noch keine Bewertungen
- Mycophenolate Mofetil (CellCept)Dokument16 SeitenMycophenolate Mofetil (CellCept)ddandan_2Noch keine Bewertungen
- Summary of Product Characteristics 1 Name of The Medicinal ProductDokument9 SeitenSummary of Product Characteristics 1 Name of The Medicinal Productddandan_2Noch keine Bewertungen
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Dokument15 SeitenIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2Noch keine Bewertungen
- Fusid®: TabletsDokument8 SeitenFusid®: Tabletsddandan_2Noch keine Bewertungen
- Product Information: Chemical StructureDokument10 SeitenProduct Information: Chemical Structureddandan_2Noch keine Bewertungen
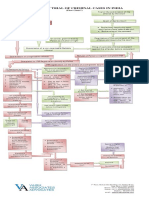
- Process of Trial of Criminal Cases in India (Flow Chart)Dokument1 SeiteProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Argumentative Essay-2Dokument4 SeitenArgumentative Essay-2api-385385980Noch keine Bewertungen
- Introduction To Strategic Cost Management and Management AccountingDokument3 SeitenIntroduction To Strategic Cost Management and Management AccountingnovyNoch keine Bewertungen
- Using Open-Ended Tools in Facilitating Mathematics and Science LearningDokument59 SeitenUsing Open-Ended Tools in Facilitating Mathematics and Science LearningDomina Jayne PagapulaanNoch keine Bewertungen
- Jamaica Sloane Conference Brochure-1Dokument4 SeitenJamaica Sloane Conference Brochure-1labrishNoch keine Bewertungen
- Physical Medicine Rehabilitation Brochure Bangkok 2020Dokument6 SeitenPhysical Medicine Rehabilitation Brochure Bangkok 2020nur yulia sariNoch keine Bewertungen
- Business Analytics Case Study - NetflixDokument2 SeitenBusiness Analytics Case Study - NetflixPurav PatelNoch keine Bewertungen
- Filed: Patrick FisherDokument12 SeitenFiled: Patrick FisherScribd Government DocsNoch keine Bewertungen
- Digitek Company Pre - QualificationDokument103 SeitenDigitek Company Pre - QualificationRey MichaelNoch keine Bewertungen
- Assignment # (02) : Abasyn University Peshawar Department of Computer ScienceDokument4 SeitenAssignment # (02) : Abasyn University Peshawar Department of Computer ScienceAndroid 360Noch keine Bewertungen
- Pineapple Working PaperDokument57 SeitenPineapple Working PaperAnonymous EAineTiz100% (7)
- List - of - Members As On 6 3 18 PDFDokument8 SeitenList - of - Members As On 6 3 18 PDFashish jaiswal100% (1)
- 20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánDokument131 Seiten20 Đề thi thử tốt nghiệp THPT năm 2021 - có đáp ánThanh NganNoch keine Bewertungen
- 77-105 Victoria Road, Landscape PlansDokument2 Seiten77-105 Victoria Road, Landscape PlansAndrew CostiNoch keine Bewertungen
- Preparatory Surface Cleaning of Architectural Sandstone: Standard Practice ForDokument2 SeitenPreparatory Surface Cleaning of Architectural Sandstone: Standard Practice Fors.swamyNoch keine Bewertungen
- 39 Storey Treehouse Activity Pack PDFDokument11 Seiten39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Bibliografia Antenas y RadioDokument3 SeitenBibliografia Antenas y RadioJorge HerreraNoch keine Bewertungen
- Strategic Cost Management: Questions For Writing and DiscussionDokument44 SeitenStrategic Cost Management: Questions For Writing and Discussionmvlg26Noch keine Bewertungen
- New Microsoft Office Word DocumentDokument3 SeitenNew Microsoft Office Word DocumentVince Vince100% (1)
- Analytical ReasoningDokument7 SeitenAnalytical ReasoningKashif NadeemNoch keine Bewertungen
- Cu 5 - The Law Enforcement Pillar Part 2Dokument22 SeitenCu 5 - The Law Enforcement Pillar Part 2marygrace.sacbibit.lawNoch keine Bewertungen
- Product Bulletin Fisher 8580 Rotary Valve en 123032Dokument16 SeitenProduct Bulletin Fisher 8580 Rotary Valve en 123032Rachmat MaulanaNoch keine Bewertungen
- English Full Book PaperDokument2 SeitenEnglish Full Book PaperSaira BatoolNoch keine Bewertungen
- Lesson 3 POWERDokument25 SeitenLesson 3 POWERLord Byron FerrerNoch keine Bewertungen
- Case Analysis OF Rajinder Singh V. State of PunjabDokument12 SeitenCase Analysis OF Rajinder Singh V. State of PunjabP TejeswariNoch keine Bewertungen
- Certificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Dokument71 SeitenCertificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Chetana YadawadNoch keine Bewertungen
- Policy ScheduleDokument1 SeitePolicy ScheduleDinesh nawaleNoch keine Bewertungen
- Charging Station Location and Sizing For Electric Vehicles Under CongestionDokument20 SeitenCharging Station Location and Sizing For Electric Vehicles Under CongestionJianli ShiNoch keine Bewertungen
- At The End of The Lesson, The Students Will Be Able To Apply The Indefinite Articles in The Given SentencesDokument11 SeitenAt The End of The Lesson, The Students Will Be Able To Apply The Indefinite Articles in The Given SentencesRhielle Dimaculangan CabañezNoch keine Bewertungen
- GO 44 RUDA ExpansionDokument4 SeitenGO 44 RUDA ExpansionbharathNoch keine Bewertungen