Das könnte Ihnen auch gefallen
- WHO List of Books, 2006Dokument161 SeitenWHO List of Books, 2006Joenabie Andoy Encanto100% (1)
- Abruptio PlacentaDokument13 SeitenAbruptio Placentamiss RN92% (12)
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Anaemia in Pregnancy: Definition and IncidenceDokument14 SeitenAnaemia in Pregnancy: Definition and IncidencejNoch keine Bewertungen
- Obg 2Dokument150 SeitenObg 2PrathibhaNoch keine Bewertungen
- ObturatorsDokument28 SeitenObturatorsDianne Mamaid100% (1)
- Anemia in PregnancyDokument53 SeitenAnemia in PregnancysyafahalimNoch keine Bewertungen
- Anemia PregnancyمحاضرةDokument33 SeitenAnemia PregnancyمحاضرةSamia Abu AishiaNoch keine Bewertungen
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Government College Nursing Anemia Nutritional DeficiencyDokument7 SeitenGovernment College Nursing Anemia Nutritional Deficiencypriyanka100% (2)
- F623Dokument8 SeitenF623Gustavo Suarez100% (1)
- Mummies: Secrets of The PharaohsDokument20 SeitenMummies: Secrets of The PharaohsNorma Aser100% (1)
- MNT I Case Study 1 Anemia in Pregnancy - XhouDokument18 SeitenMNT I Case Study 1 Anemia in Pregnancy - Xhouapi-254534492100% (1)
- Anaemia in PregnancyDokument35 SeitenAnaemia in PregnancyUmar Dhani89% (9)
- Anemia in PregnancyDokument9 SeitenAnemia in PregnancyShalini Shanmugalingam100% (1)
- Excerpt: "Birth Matters" by Ina May GaskinDokument16 SeitenExcerpt: "Birth Matters" by Ina May Gaskinwamu885100% (1)
- Anemia in PregnancyDokument20 SeitenAnemia in PregnancyMargaretha UsbokoNoch keine Bewertungen
- Government College of Nursing: JodhpurDokument9 SeitenGovernment College of Nursing: JodhpurpriyankaNoch keine Bewertungen
- Management of Anaemia in PregnancyDokument8 SeitenManagement of Anaemia in PregnancyAnonymous 9dVZCnTXSNoch keine Bewertungen
- Bu Elda PrintDokument14 SeitenBu Elda PrintDian Soekmawaty Riezqy AriendhaNoch keine Bewertungen
- SA Anemia PregnancyDokument10 SeitenSA Anemia PregnancyPujanaWiaktaNoch keine Bewertungen
- SOGP AnaemiaDokument16 SeitenSOGP AnaemiaMuhammad Farrukh ul IslamNoch keine Bewertungen
- Uk Guidelines Iron Deficiency in PregnancyDokument34 SeitenUk Guidelines Iron Deficiency in PregnancyFirdaus AzinunNoch keine Bewertungen
- RTC-SW 2014 10 P Anaemia in Pregnancy GuidelineDokument5 SeitenRTC-SW 2014 10 P Anaemia in Pregnancy GuidelineShiina LeeNoch keine Bewertungen
- Anemia in Pregnancy: Causes, Effects and TreatmentDokument6 SeitenAnemia in Pregnancy: Causes, Effects and TreatmentLeroy LoyNoch keine Bewertungen
- 2012 UK Guidelines On The Management of Iron Deficiency in Pregnancy - Pavord - 2012 - British Journal of Haematology - Wiley Online LibraryDokument19 Seiten2012 UK Guidelines On The Management of Iron Deficiency in Pregnancy - Pavord - 2012 - British Journal of Haematology - Wiley Online LibraryKedokteran Fetomaternal SurabayaNoch keine Bewertungen
- UK Guidelines Iron Deficiency in Pregnancy PDFDokument34 SeitenUK Guidelines Iron Deficiency in Pregnancy PDFYoga Rhamada SiregarNoch keine Bewertungen
- AnemiaDokument11 SeitenAnemiadewiq_wahyuNoch keine Bewertungen
- Buy The Book PDA Download: Update MeDokument12 SeitenBuy The Book PDA Download: Update MeyanajaeNoch keine Bewertungen
- AnaemiaDokument66 SeitenAnaemiaSusmita DasNoch keine Bewertungen
- Anaemia in Pregnancy - RFDokument29 SeitenAnaemia in Pregnancy - RFTiger DsixtytwoNoch keine Bewertungen
- Anemia in Pregnancy GuideDokument7 SeitenAnemia in Pregnancy GuideLenrok AdrianNoch keine Bewertungen
- Disampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Dokument46 SeitenDisampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Asis muhammadNoch keine Bewertungen
- Anaemia in PregnancyDokument76 SeitenAnaemia in PregnancysivaNoch keine Bewertungen
- Anemia in Pregnancy: Causes, Types, Symptoms, Treatment and PreventionDokument4 SeitenAnemia in Pregnancy: Causes, Types, Symptoms, Treatment and PreventionsupermilyNoch keine Bewertungen
- Boston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Dokument4 SeitenBoston Medical Center Maternity Care Guideline Guideline: Iron Defficiency Anemia Accepted: Updated: 04/2015Fernando Cardenas AriasNoch keine Bewertungen
- Clinical Update: Anemia in PregnancyDokument4 SeitenClinical Update: Anemia in PregnancyAnisah TifaniNoch keine Bewertungen
- BJH 9012Dokument13 SeitenBJH 9012ooiziungieNoch keine Bewertungen
- Anemia in PregnancyDokument11 SeitenAnemia in PregnancyIcetea KokomNoch keine Bewertungen
- Anemia in PregnancyDokument4 SeitenAnemia in PregnancyDheyaa A. SabahNoch keine Bewertungen
- Anemia During PregnancyDokument15 SeitenAnemia During PregnancyKuleshwar SahuNoch keine Bewertungen
- Case Questions TranscriptDokument7 SeitenCase Questions TranscriptSa7arNoch keine Bewertungen
- During PregnancyDokument31 SeitenDuring PregnancyMotaz AliNoch keine Bewertungen
- Give The Name of Different Forms of Anemia With TreatmentDokument6 SeitenGive The Name of Different Forms of Anemia With TreatmentRaju DasNoch keine Bewertungen
- Pregnancy Anemia Types and ManagementDokument23 SeitenPregnancy Anemia Types and ManagementsuperjaxxxonNoch keine Bewertungen
- Dr. Ramya Moderator: DR - PallaveeDokument71 SeitenDr. Ramya Moderator: DR - PallaveeMonika shankarNoch keine Bewertungen
- Case Study 2 Nutrition FinalDokument10 SeitenCase Study 2 Nutrition Finalapi-271149361Noch keine Bewertungen
- Hypocalcemia in The NewbornDokument5 SeitenHypocalcemia in The NewbornrenjithNoch keine Bewertungen
- Anemia in PregnancyDokument14 SeitenAnemia in PregnancyWern Ching Lee50% (2)
- Orig 1 S 040 LBLDokument7 SeitenOrig 1 S 040 LBLpatgarettNoch keine Bewertungen
- Anaemia in Pregnancy GuideDokument33 SeitenAnaemia in Pregnancy GuideKomal Dhulap100% (1)
- MBBS-4 No014089Dokument38 SeitenMBBS-4 No014089diphylleia90grayiNoch keine Bewertungen
- Anaemia in PregnancyDokument31 SeitenAnaemia in PregnancyheatherNoch keine Bewertungen
- 01.anaemia in PregnancyDokument29 Seiten01.anaemia in PregnancyMtwe ZakayoNoch keine Bewertungen
- Therapeutic Choices 2011Dokument1.365 SeitenTherapeutic Choices 2011priyarajan007Noch keine Bewertungen
- Manchester Anaemia GuideDokument13 SeitenManchester Anaemia Guidemubzy14Noch keine Bewertungen
- Anemia Defisiensi Pada KehamilanDokument23 SeitenAnemia Defisiensi Pada KehamilanAmri AshshiddieqNoch keine Bewertungen
- ObsNGyn - Medical Disorders in Pregnancy AtfDokument15 SeitenObsNGyn - Medical Disorders in Pregnancy Atfosman nurNoch keine Bewertungen
- SIM - Anemias of PregnancyDokument17 SeitenSIM - Anemias of PregnancyGabrielle EvangelistaNoch keine Bewertungen
- Anemia in Pregnancy: Causes, Symptoms, Diagnosis and TreatmentDokument5 SeitenAnemia in Pregnancy: Causes, Symptoms, Diagnosis and TreatmentDavidNoch keine Bewertungen
- Anemia in Pregnancy PDFDokument5 SeitenAnemia in Pregnancy PDFDavidNoch keine Bewertungen
- Anemia and Pregnancy: Sunil Kumar DahaDokument43 SeitenAnemia and Pregnancy: Sunil Kumar DahaBhawna JoshiNoch keine Bewertungen
- Approaches To Anemia in Pregnancy: Research and ReviewsDokument5 SeitenApproaches To Anemia in Pregnancy: Research and ReviewsRahulAcharyaNoch keine Bewertungen
- Anemia in Pregnancy: Causes, Diagnosis and ManagementDokument17 SeitenAnemia in Pregnancy: Causes, Diagnosis and Managementvictor onapaNoch keine Bewertungen
- Iron Deficiency Anemia.1Dokument21 SeitenIron Deficiency Anemia.1Rumaisa AbdullahNoch keine Bewertungen
- The #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandVon EverandThe #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandNoch keine Bewertungen
- Compare leading SA medical schemes' primary healthcare benefitsDokument5 SeitenCompare leading SA medical schemes' primary healthcare benefitsMNQOBINoch keine Bewertungen
- pedCAT Product InformationDokument2 SeitenpedCAT Product InformationVinti SinghNoch keine Bewertungen
- هااامDokument2 SeitenهااامEsamNoch keine Bewertungen
- Claim Form for Outpatient & Dental BenefitsDokument1 SeiteClaim Form for Outpatient & Dental BenefitsYiki TanNoch keine Bewertungen
- Obstetrics, Gynaecology and Reproductive Medicine: Editor-in-ChiefDokument33 SeitenObstetrics, Gynaecology and Reproductive Medicine: Editor-in-ChiefRaed Q. N. NazzalNoch keine Bewertungen
- NASC 4 Fact or BluffDokument33 SeitenNASC 4 Fact or BluffJona MangabanNoch keine Bewertungen
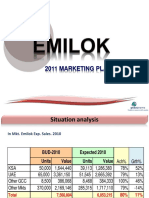
- Emilok 2011 MKT PlanDokument19 SeitenEmilok 2011 MKT Planmaawi2002yahoocomNoch keine Bewertungen
- The Rol of ParamedicsDokument7 SeitenThe Rol of ParamedicsJean ColqueNoch keine Bewertungen
- Clinical Exam of Thorax, Abdomen and PelvisDokument42 SeitenClinical Exam of Thorax, Abdomen and PelvisTunnelssNoch keine Bewertungen
- Rita Alcaraz: Clinical Experience and SkillsDokument1 SeiteRita Alcaraz: Clinical Experience and Skillsapi-398600648Noch keine Bewertungen
- Terminology in Clinical SettingDokument13 SeitenTerminology in Clinical SettingCiuss ThamrinNoch keine Bewertungen
- Visual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractDokument8 SeitenVisual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractElyani RahmanNoch keine Bewertungen
- OPTIKON 2000 OPHTHALMIC EQUIPMENT CATALOGDokument7 SeitenOPTIKON 2000 OPHTHALMIC EQUIPMENT CATALOGhelpurusNoch keine Bewertungen
- Schedule of Charges-Holy Family - Sep 08Dokument64 SeitenSchedule of Charges-Holy Family - Sep 08Quirinevv100% (1)
- FrenectomiaDokument8 SeitenFrenectomiaRafa LopezNoch keine Bewertungen
- Uterinefibroids 130120064643 Phpapp02Dokument73 SeitenUterinefibroids 130120064643 Phpapp02Tharun KumarNoch keine Bewertungen
- Neuromonitoreo 2014Dokument21 SeitenNeuromonitoreo 2014Marco CaranguiNoch keine Bewertungen
- Air Travel in PregnancyDokument2 SeitenAir Travel in PregnancyDiana HalimNoch keine Bewertungen
- Management For RDSDokument85 SeitenManagement For RDSNurhafizoh HussinNoch keine Bewertungen
- Osteosintesis Ortognatica MandibulaDokument41 SeitenOsteosintesis Ortognatica MandibulaMaria Mercedes Rosales NuñezNoch keine Bewertungen
- Guidelines For Obstetric Epidural Blood Patch NPS 5.4.06Dokument2 SeitenGuidelines For Obstetric Epidural Blood Patch NPS 5.4.06grigmihNoch keine Bewertungen
- Dental pulp exposures in germ-free and conventional ratsDokument10 SeitenDental pulp exposures in germ-free and conventional ratsValentina Llanca MejíasNoch keine Bewertungen
- UG Assessment Form AIIDokument39 SeitenUG Assessment Form AIIdrpklalNoch keine Bewertungen
- CairoDentalJournal14 23 26 1998Dokument4 SeitenCairoDentalJournal14 23 26 1998Norman Onyx Tardo DagangNoch keine Bewertungen