Das könnte Ihnen auch gefallen
- Training Needs AssessmentDokument11 SeitenTraining Needs AssessmentKarina Madriaga100% (1)
- Sexually Transmitted DiseasesDokument174 SeitenSexually Transmitted DiseasesfroizkiNoch keine Bewertungen
- G2A Glitch DONT LEAK 2Dokument7 SeitenG2A Glitch DONT LEAK 2qDeficiencyNoch keine Bewertungen
- Practical CS ProcessingDokument483 SeitenPractical CS ProcessinganAMUstudent100% (2)
- Simple Love Spells That WorkDokument14 SeitenSimple Love Spells That Workagg24ankitNoch keine Bewertungen
- Anemia in PregnancyDokument9 SeitenAnemia in PregnancyKarina Madriaga100% (2)
- Drill Bit Classifier 2004 PDFDokument15 SeitenDrill Bit Classifier 2004 PDFgustavoemir0% (2)
- Kawasaki DiseaseDokument14 SeitenKawasaki Diseaseken100% (2)
- MeningitisDokument23 SeitenMeningitisPutri RamadhaniNoch keine Bewertungen
- Leptospirosis FinalDokument5 SeitenLeptospirosis FinalufrieNoch keine Bewertungen
- Combat Storm - Shipping ContainerDokument6 SeitenCombat Storm - Shipping ContainermoiNoch keine Bewertungen
- Volleyball Unit PlanDokument4 SeitenVolleyball Unit Planapi-214597204Noch keine Bewertungen
- Caterpillar Sis (01.2014) MultilanguageDokument10 SeitenCaterpillar Sis (01.2014) MultilanguageTemmy Candra Wijaya100% (1)
- Rheumatoid ArthritisDokument52 SeitenRheumatoid ArthritisSophia Veron100% (2)
- Infections During PregnancyDokument9 SeitenInfections During PregnancyKarina Madriaga100% (4)
- Scale Aircraft Modelling 01.2019Dokument100 SeitenScale Aircraft Modelling 01.2019Nikko LimuaNoch keine Bewertungen
- Family Nursing Care PlanDokument3 SeitenFamily Nursing Care PlanAlexa Abidin Oldenborg96% (28)
- Kawasaki's DiseaseDokument3 SeitenKawasaki's DiseaseDavid ChengNoch keine Bewertungen
- Rheumatic FeverDokument26 SeitenRheumatic FeverAhmed Ben Bella100% (2)
- The Challenge of Managing Tendinopathy in Competing AthletesDokument7 SeitenThe Challenge of Managing Tendinopathy in Competing AthletesMichele MarengoNoch keine Bewertungen
- Vasculitis in ChildrenDokument22 SeitenVasculitis in ChildrenRashed ShatnawiNoch keine Bewertungen
- Dengue Fever Is A MosquitoDokument4 SeitenDengue Fever Is A MosquitoPartha Permana PutraNoch keine Bewertungen
- Rheumatic Heart DiseaseDokument13 SeitenRheumatic Heart Diseasedy15Noch keine Bewertungen
- Kawasaki DiseaseDokument9 SeitenKawasaki DiseaseMery Rose GanitnitNoch keine Bewertungen
- Republic of The Philippines Tarlac State University College of Nursing Graduate Studies ProgramDokument9 SeitenRepublic of The Philippines Tarlac State University College of Nursing Graduate Studies ProgramCorinthiaMaeMarceloNoch keine Bewertungen
- CasestudyDokument223 SeitenCasestudyDrAbhilash RMNoch keine Bewertungen
- Scleroderma, Sjogren's SyndromeDokument31 SeitenScleroderma, Sjogren's SyndromeSalomeSibashviliNoch keine Bewertungen
- Q PathoDokument5 SeitenQ PathoEunice Erika NebalascaNoch keine Bewertungen
- Lecture: Erysipelas: Basic Clinical PrinciplesDokument15 SeitenLecture: Erysipelas: Basic Clinical PrinciplesIsak ShatikaNoch keine Bewertungen
- DDX Chart Part 1Dokument5 SeitenDDX Chart Part 1M.DalaniNoch keine Bewertungen
- Infomercial ScriptDokument5 SeitenInfomercial ScriptZAPA OfficialNoch keine Bewertungen
- Acute Rheumatic Fever ARFDokument83 SeitenAcute Rheumatic Fever ARFKhaled SakrNoch keine Bewertungen
- Lepto SpirosDokument6 SeitenLepto SpirosMar OrdanzaNoch keine Bewertungen
- Rheumatic DiseasesDokument42 SeitenRheumatic DiseasesToko RaMy LineNoch keine Bewertungen
- Endocrine System DisorderDokument16 SeitenEndocrine System DisorderAnonymous KnlqfUtNoch keine Bewertungen
- Topic 18. Rheumatic DiaseasesDokument8 SeitenTopic 18. Rheumatic DiaseasesAdeleye John AdebolaNoch keine Bewertungen
- 1 - Rheumatic Fever and Valvular Diseases (Summary and MCQS)Dokument12 Seiten1 - Rheumatic Fever and Valvular Diseases (Summary and MCQS)فرقان سلام عيسى عبدNoch keine Bewertungen
- Read The Text and Write The Name of The Disease. Disease SymptomsDokument3 SeitenRead The Text and Write The Name of The Disease. Disease SymptomsGabby SOolisNoch keine Bewertungen
- A Simple Guide to Mucocutaneous Lymph Node Syndrome (Kawasaki Disease), Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Mucocutaneous Lymph Node Syndrome (Kawasaki Disease), Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- What Is HenochDokument7 SeitenWhat Is HenochHazel Monique SaysonNoch keine Bewertungen
- Rheumatic Fever and RHDDokument49 SeitenRheumatic Fever and RHDbereket gashuNoch keine Bewertungen
- Kawasaki DiseaseDokument24 SeitenKawasaki DiseaseNikki AutenticoNoch keine Bewertungen
- Rheumatic Heart Disease IntroDokument3 SeitenRheumatic Heart Disease IntroTrexy LozanoNoch keine Bewertungen
- Juvenile Rheumatoid ArthritisDokument10 SeitenJuvenile Rheumatoid ArthritisIsak ShatikaNoch keine Bewertungen
- Ray Um ADokument6 SeitenRay Um AE_jay_Gusago_1951Noch keine Bewertungen
- Pediatrics Larg SlidesDokument130 SeitenPediatrics Larg SlidesObada DyabNoch keine Bewertungen
- Fever Synonym:: Modes of TransmissionDokument6 SeitenFever Synonym:: Modes of TransmissionEjie Boy IsagaNoch keine Bewertungen
- KawasakiDokument28 SeitenKawasakiLaith DmourNoch keine Bewertungen
- Infectious Diseases That Evolve With ExanthemaDokument64 SeitenInfectious Diseases That Evolve With ExanthemaBeni KelnerNoch keine Bewertungen
- Rheumatic Fever: DR: Kaem Shir AliDokument24 SeitenRheumatic Fever: DR: Kaem Shir AliMwanja Moses100% (1)
- 1 Rheumatic Fever and RHDDokument53 Seiten1 Rheumatic Fever and RHDDanny DesuNoch keine Bewertungen
- Patient Education - Systemic Lupus Erythematosus (Beyond The Basics) - UpToDateDokument14 SeitenPatient Education - Systemic Lupus Erythematosus (Beyond The Basics) - UpToDatepakiza noorNoch keine Bewertungen
- September 2005 UpdateDokument19 SeitenSeptember 2005 UpdateAkbar Rizki ArNoch keine Bewertungen
- Topics For Oral Exam TTKawasakiFIDokument3 SeitenTopics For Oral Exam TTKawasakiFIPCRMNoch keine Bewertungen
- English For Nursing StudentDokument11 SeitenEnglish For Nursing StudentAriel MNoch keine Bewertungen
- Top Ten Disease in BandungDokument10 SeitenTop Ten Disease in BandungSaarah Thifal AiniNoch keine Bewertungen
- Septic Shock NCLEX ReviewDokument5 SeitenSeptic Shock NCLEX Reviewnmukila2Noch keine Bewertungen
- ValvularHeartDisease Notes S5w4Dokument6 SeitenValvularHeartDisease Notes S5w4razzletothedazzleNoch keine Bewertungen
- M13 v2 Dermatology & STI - LO5Dokument6 SeitenM13 v2 Dermatology & STI - LO5medipro clinicNoch keine Bewertungen
- Microbio Skin and Eyes LectureDokument30 SeitenMicrobio Skin and Eyes LecturesweetiepotamusNoch keine Bewertungen
- 1) DIABETES TYPE 2: Diabetes Is A Condition in Which The Body Cannot ProperlyDokument3 Seiten1) DIABETES TYPE 2: Diabetes Is A Condition in Which The Body Cannot ProperlyMonica SandharNoch keine Bewertungen
- Signs and Symptoms of Leprosy and SchistosomiasisDokument3 SeitenSigns and Symptoms of Leprosy and SchistosomiasisRheimon Jay Abuan BalcitaNoch keine Bewertungen
- Kelainan Kepala Dan LeherDokument17 SeitenKelainan Kepala Dan LeherSoraya HumairaNoch keine Bewertungen
- Anatomy ActivityDokument2 SeitenAnatomy Activityjonar parinasNoch keine Bewertungen
- BLS - The Detailed Online Five GuideDokument23 SeitenBLS - The Detailed Online Five GuidepeterNoch keine Bewertungen
- g7 NCD 200209062226Dokument44 Seiteng7 NCD 200209062226Nanette Orenciano MedinaNoch keine Bewertungen
- Gastroenteritis: Chronic Renal FailureDokument4 SeitenGastroenteritis: Chronic Renal FailureJohnhineNoch keine Bewertungen
- AlyssaDokument2 SeitenAlyssaJo Li NaNoch keine Bewertungen
- Henoch-Schonlein Purpura Clinical Presentation History, Physical Examination, ComplicationsDokument19 SeitenHenoch-Schonlein Purpura Clinical Presentation History, Physical Examination, ComplicationsResty SukurNoch keine Bewertungen
- Kuliah Pakar Modul 3.1Dokument68 SeitenKuliah Pakar Modul 3.1Pramesti DarojahNoch keine Bewertungen
- A Report On Dengue Hemorrhagic Fever: Submitted byDokument6 SeitenA Report On Dengue Hemorrhagic Fever: Submitted byEjay ObarNoch keine Bewertungen
- Burns Blood Transfusion PancreatitisDokument4 SeitenBurns Blood Transfusion PancreatitisKath DeguzmanNoch keine Bewertungen
- Inflamed Blood Vessels (Vasculitis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandInflamed Blood Vessels (Vasculitis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Goal Met.: Polymorphonuclea R LeukocytesDokument2 SeitenGoal Met.: Polymorphonuclea R LeukocytesKarina MadriagaNoch keine Bewertungen
- NCM 113 - Timeline of TopicsDokument8 SeitenNCM 113 - Timeline of TopicsKarina MadriagaNoch keine Bewertungen
- Drug StudyDokument60 SeitenDrug StudyKarina MadriagaNoch keine Bewertungen
- Risk For Decreased Cardiac Tissue PerfusionDokument3 SeitenRisk For Decreased Cardiac Tissue PerfusionKarina MadriagaNoch keine Bewertungen
- Activity 4Dokument1 SeiteActivity 4Karina MadriagaNoch keine Bewertungen
- Activity 5 Community Health Care ProcessDokument16 SeitenActivity 5 Community Health Care ProcessKarina MadriagaNoch keine Bewertungen
- Mucocutaneous Lymph Node SyndromeDokument9 SeitenMucocutaneous Lymph Node SyndromeKarina MadriagaNoch keine Bewertungen
- Midterms Group 5Dokument25 SeitenMidterms Group 5Karina MadriagaNoch keine Bewertungen
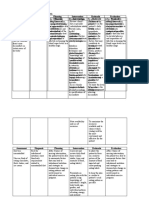
- NCPsDokument3 SeitenNCPsKarina MadriagaNoch keine Bewertungen
- Beatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesDokument2 SeitenBeatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesKarina MadriagaNoch keine Bewertungen
- Beatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesDokument2 SeitenBeatitudes Beatitudes As Enshrined in The Filipino Character Reversal of The Beatitudes/ DisvaluesKarina MadriagaNoch keine Bewertungen
- FreedomDokument1 SeiteFreedomKarina MadriagaNoch keine Bewertungen
- Prenatal Care Common Discomforts During PregnancyDokument5 SeitenPrenatal Care Common Discomforts During PregnancyKarina MadriagaNoch keine Bewertungen
- JusticeDokument3 SeitenJusticeKarina MadriagaNoch keine Bewertungen
- August 14Dokument2 SeitenAugust 14Karina MadriagaNoch keine Bewertungen
- Assignment For BSN 3 - A - RLEDokument2 SeitenAssignment For BSN 3 - A - RLEKarina Madriaga100% (1)
- NonmaleficenceDokument3 SeitenNonmaleficenceKarina MadriagaNoch keine Bewertungen
- Nutrition and Bone Health: Group 6Dokument22 SeitenNutrition and Bone Health: Group 6Karina MadriagaNoch keine Bewertungen
- Official View Similarities Popular ViewDokument1 SeiteOfficial View Similarities Popular ViewKarina MadriagaNoch keine Bewertungen
- Human Person: The Key of Moral Life The Agent of Morality: Gmail-Jpico@spup - Edu.phDokument2 SeitenHuman Person: The Key of Moral Life The Agent of Morality: Gmail-Jpico@spup - Edu.phKarina MadriagaNoch keine Bewertungen
- GEC 109 August 15Dokument1 SeiteGEC 109 August 15Karina MadriagaNoch keine Bewertungen
- Community Organizing Participatory Action ResearchDokument8 SeitenCommunity Organizing Participatory Action ResearchKarina MadriagaNoch keine Bewertungen
- Lesson 2Dokument6 SeitenLesson 2Karina MadriagaNoch keine Bewertungen
- Official View Similarities Popular ViewDokument1 SeiteOfficial View Similarities Popular ViewKarina MadriagaNoch keine Bewertungen
- Lesson-1 3Dokument14 SeitenLesson-1 3Karina MadriagaNoch keine Bewertungen
- Grammar Review A2-B1Dokument5 SeitenGrammar Review A2-B1Lena Silva SouzaNoch keine Bewertungen
- Department of Labor: BC Retaining Wall CodeDokument2 SeitenDepartment of Labor: BC Retaining Wall CodeUSA_DepartmentOfLaborNoch keine Bewertungen
- Piezoelectric-Material Based Energy Harvesting Device.Dokument29 SeitenPiezoelectric-Material Based Energy Harvesting Device.jobert100% (1)
- 7 ApportionmentDokument46 Seiten7 Apportionmentsass sofNoch keine Bewertungen
- JHS Integrated Science Preamble, Jan 2012 - FinalDokument15 SeitenJHS Integrated Science Preamble, Jan 2012 - Finalfrank adamsNoch keine Bewertungen
- MELASMA (Ardy, Kintan, Fransisca)Dokument20 SeitenMELASMA (Ardy, Kintan, Fransisca)Andi Firman MubarakNoch keine Bewertungen
- CR-805 Retransfer PrinterDokument2 SeitenCR-805 Retransfer PrinterBolivio FelizNoch keine Bewertungen
- Introduction To Physiotherapy PracticeDokument22 SeitenIntroduction To Physiotherapy PracticejNoch keine Bewertungen
- K To 12 Math 7 Curriculum Guide PDFDokument15 SeitenK To 12 Math 7 Curriculum Guide PDFEdmar Tan Fabi100% (1)
- Victaulic-FP-FireLock Fire-Pac Series 745 PreactionDokument9 SeitenVictaulic-FP-FireLock Fire-Pac Series 745 PreactionTấn ĐạtNoch keine Bewertungen
- SalerioDokument28 SeitenSalerioRizqaFebrilianyNoch keine Bewertungen
- Biography of Anna HazareDokument4 SeitenBiography of Anna HazareGenesis FirstNoch keine Bewertungen
- Review Systems of Linear Equations All MethodsDokument4 SeitenReview Systems of Linear Equations All Methodsapi-265647260Noch keine Bewertungen
- Appendicitis Case StudyDokument6 SeitenAppendicitis Case StudyKimxi Chiu LimNoch keine Bewertungen
- UniFi Quick GuideDokument2 SeitenUniFi Quick GuideAndhika TharunaNoch keine Bewertungen
- Van Daley - Leadership ResumeDokument1 SeiteVan Daley - Leadership Resumeapi-352146181Noch keine Bewertungen
- FL Switch 2000Dokument124 SeitenFL Switch 2000marcosNoch keine Bewertungen
- Case Study Presentation - CGDokument37 SeitenCase Study Presentation - CGapi-290866384Noch keine Bewertungen
- RSM222.f22.CourseOutline v3 2022-09-05Dokument9 SeitenRSM222.f22.CourseOutline v3 2022-09-05Kirsten WangNoch keine Bewertungen
- Test Cases: Project Name: Virtual ClassroomDokument5 SeitenTest Cases: Project Name: Virtual ClassroomTina HernandezNoch keine Bewertungen
- SOP For Operation & Calibration of PH Meter - QualityGuidancesDokument9 SeitenSOP For Operation & Calibration of PH Meter - QualityGuidancesfawaz khalilNoch keine Bewertungen