Appendix 40
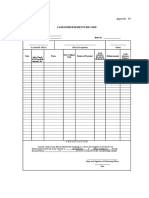
CASH DISBURSEMENTS RECORD
Entity Name : __________________________
Fund Cluster : __________________________ Sheet No. : _________________
___________________ ________________________________ ________________
Accountable Officer Official Designation Station
Cash
Cash
UACS Object Advance
Date Payee Nature of Payment Disbursements Advance
ADA/Check/ Code Received/
Balance
DV/Payroll/R (Refunded)
eference No.
CERTIFICATION
I hereby certify on my official oath that the foregoing is a correct and complete record of all cash
disbursements had by me in my capacity as ______(Designation)____ of (Name of Agency) during
the period from _______________ to _______________,inclusive, as indicated in the corresponding columns.
_______________________________
Name and Signature of Disbursing Officer
________________
Date
110
Das könnte Ihnen auch gefallen
- AOM 2023-004 Understated Due To NGADokument4 SeitenAOM 2023-004 Understated Due To NGAKean Fernand BocaboNoch keine Bewertungen
- Accounting For Disbursements and Related TransactionsDokument12 SeitenAccounting For Disbursements and Related TransactionsJustine GuilingNoch keine Bewertungen
- Commission On Audit: of FQR L) IqilippiursDokument3 SeitenCommission On Audit: of FQR L) IqilippiursDianeNoch keine Bewertungen
- LGU-NGAS TableofContentsVol1Dokument6 SeitenLGU-NGAS TableofContentsVol1Pee-Jay Inigo UlitaNoch keine Bewertungen
- MC 2018-034 - Updated Guidelines On RATADokument7 SeitenMC 2018-034 - Updated Guidelines On RATAKarla KatigbakNoch keine Bewertungen
- Liquidation FormsDokument9 SeitenLiquidation FormsMark Patrics Comentan VerderaNoch keine Bewertungen
- Korean Business Dictionary: American and Korean Business Terms for the Internet AgeVon EverandKorean Business Dictionary: American and Korean Business Terms for the Internet AgeNoch keine Bewertungen
- Sworn Statements Format v042513 FoundationDokument15 SeitenSworn Statements Format v042513 FoundationJohn Paul Aurellano100% (1)
- Certification of Travel CompletedDokument2 SeitenCertification of Travel CompletedLourdes UrgellesNoch keine Bewertungen
- Appendix 46 RERDokument1 SeiteAppendix 46 RERWinston Yuta100% (2)
- RMC 130-2016Dokument2 SeitenRMC 130-2016Earl John PajaroNoch keine Bewertungen
- NGAS Illustrative Accounting EntriesDokument9 SeitenNGAS Illustrative Accounting EntriesDaniel OngNoch keine Bewertungen
- San Pablo City Water District Laguna Executive Summary 2021 PDFDokument8 SeitenSan Pablo City Water District Laguna Executive Summary 2021 PDFJohn Archie SerranoNoch keine Bewertungen
- AMLA GuidelineDokument54 SeitenAMLA Guidelineeliasox123100% (1)
- Audit of Confidential Fund of LGUDokument16 SeitenAudit of Confidential Fund of LGUBarwin Scott VillordonNoch keine Bewertungen
- Journal Entry Voucher: Municipal Government of Lambunao Disbursement VoucherDokument12 SeitenJournal Entry Voucher: Municipal Government of Lambunao Disbursement VoucherFrancisco Lubas Santillana IVNoch keine Bewertungen
- Statement of Ongoing Contracts - 0Dokument1 SeiteStatement of Ongoing Contracts - 0Jessabelle RamosNoch keine Bewertungen
- GAM Inventory PresentationDokument22 SeitenGAM Inventory PresentationRobert CastilloNoch keine Bewertungen
- Appendix 34 - CHECKS AND ADVICES TO DEBIT ACCOUNT DISBURSEMENTS RECORDDokument1 SeiteAppendix 34 - CHECKS AND ADVICES TO DEBIT ACCOUNT DISBURSEMENTS RECORDPau PerezNoch keine Bewertungen
- GAM Forms 2016Dokument27 SeitenGAM Forms 2016Grace Dela CruzNoch keine Bewertungen
- Appendix 28 - Instructions - CAFOADokument1 SeiteAppendix 28 - Instructions - CAFOAhehehedontmind meNoch keine Bewertungen
- Appendix 35 - LR Liquidation ReportDokument1 SeiteAppendix 35 - LR Liquidation ReportEtchel Osiam AvilaNoch keine Bewertungen
- Invoice Receipt For Property Form GF 30 A 2Dokument1 SeiteInvoice Receipt For Property Form GF 30 A 2Rexis ReginanNoch keine Bewertungen
- 08 BLGUMAGSAYSAYHILL 2022 AAR Part2 Findings and RecommendationsDokument22 Seiten08 BLGUMAGSAYSAYHILL 2022 AAR Part2 Findings and RecommendationsGil DavinNoch keine Bewertungen
- Report of Check Issued RCIDokument2 SeitenReport of Check Issued RCIArnie Jean AbianNoch keine Bewertungen
- Enhanced Engas and Ebudget System Version 2.0 (Ppsas and Rca Compliant) For Local Government UnitDokument5 SeitenEnhanced Engas and Ebudget System Version 2.0 (Ppsas and Rca Compliant) For Local Government UnitJayden CruzNoch keine Bewertungen
- A.8 Report On The Physical Count of Semi Expendable PropertyDokument9 SeitenA.8 Report On The Physical Count of Semi Expendable Propertyjaypee raguroNoch keine Bewertungen
- Annex C Application Form and Checklist of RequirementsDokument4 SeitenAnnex C Application Form and Checklist of RequirementsEdcel John Minglana LamanilaoNoch keine Bewertungen
- Letter of Introduction (LDDAP-ADA)Dokument1 SeiteLetter of Introduction (LDDAP-ADA)Glenda MacatangayNoch keine Bewertungen
- Appendix 30 - Instructions - RANCADokument1 SeiteAppendix 30 - Instructions - RANCApdmu regionixNoch keine Bewertungen
- Sworn Declaration of Gross Sales (LGU)Dokument1 SeiteSworn Declaration of Gross Sales (LGU)Kathyrn Ang-ZarateNoch keine Bewertungen
- Audit Report - TuburanDokument87 SeitenAudit Report - TuburanMaria100% (1)
- UACS ManualDokument41 SeitenUACS ManualHammurabi BugtaiNoch keine Bewertungen
- Sample DV PER EXPENSEDokument14 SeitenSample DV PER EXPENSEJohn Ray VelascoNoch keine Bewertungen
- Property Transfer Report: Entity Name: Fund ClusterDokument2 SeitenProperty Transfer Report: Entity Name: Fund ClusterCatherine BenbanNoch keine Bewertungen
- SSS Handbook PDFDokument45 SeitenSSS Handbook PDFsarahNoch keine Bewertungen
- LipaCity2017 Audit ReportDokument255 SeitenLipaCity2017 Audit ReportMerlo Sebasthian SilvaNoch keine Bewertungen
- Appendix 49 - Instructions - RPPCVDokument1 SeiteAppendix 49 - Instructions - RPPCVCENTRAL OFFICE ACCOUNTINGNoch keine Bewertungen
- Republic Act 9520 - CDADokument27 SeitenRepublic Act 9520 - CDAEdi wow WowNoch keine Bewertungen
- Annex 11-Logbook of Checks Issued and CancelledDokument3 SeitenAnnex 11-Logbook of Checks Issued and CancelledVermon JayNoch keine Bewertungen
- Republic of The Philippines Application For: National Water Resources Board Renewal ofDokument2 SeitenRepublic of The Philippines Application For: National Water Resources Board Renewal ofMark PesiganNoch keine Bewertungen
- The New Government Accounting System Manual For Local Government Units Chapter 1. IntroductionDokument34 SeitenThe New Government Accounting System Manual For Local Government Units Chapter 1. IntroductionaisahNoch keine Bewertungen
- Registry of Allotments and Notice of Transfer of Allocation: Appendix 31Dokument1 SeiteRegistry of Allotments and Notice of Transfer of Allocation: Appendix 31Tesa GDNoch keine Bewertungen
- TOS RFBT RevisedDokument4 SeitenTOS RFBT RevisedmadbolivarNoch keine Bewertungen
- COA CIRCULAR NO. 2024 006 March 14 2024Dokument21 SeitenCOA CIRCULAR NO. 2024 006 March 14 2024Jen IgnacioNoch keine Bewertungen
- SAOR 2015 Additional AOM DO ZDNDokument9 SeitenSAOR 2015 Additional AOM DO ZDNrussel1435Noch keine Bewertungen
- 2307Dokument16 Seiten2307Marjorie JotojotNoch keine Bewertungen
- Tax Update RR 18-2012Dokument32 SeitenTax Update RR 18-2012johamarz6245Noch keine Bewertungen
- Checklist ReliefDokument1 SeiteChecklist ReliefRobehgene Atud-JavinarNoch keine Bewertungen
- CPCS 2021-009 Grant of 3 Yr Authorized Allowances, Benefits and IncentivesDokument3 SeitenCPCS 2021-009 Grant of 3 Yr Authorized Allowances, Benefits and IncentivesEdson Jude DonosoNoch keine Bewertungen
- CAR 2D Expanded Engagement Ltr-Compilation (5-17)Dokument8 SeitenCAR 2D Expanded Engagement Ltr-Compilation (5-17)Andy RossNoch keine Bewertungen
- AAO Electronic Online System Form - 18mar2021-1Dokument1 SeiteAAO Electronic Online System Form - 18mar2021-1CherryMaeRamirezAustinNoch keine Bewertungen
- RCA LocalDokument25 SeitenRCA LocalAcu Z MarcusNoch keine Bewertungen
- Elpidio Vega Vs Joy LegaspiDokument13 SeitenElpidio Vega Vs Joy LegaspiElpidioVegaNoch keine Bewertungen
- DPWH Overtime PayDokument7 SeitenDPWH Overtime PayTarhata KalimNoch keine Bewertungen
- Cash Disbursements Record: Appendix 40Dokument1 SeiteCash Disbursements Record: Appendix 40Hike and Surf LivingNoch keine Bewertungen
- Appendix 34 - CkADADRecDokument1 SeiteAppendix 34 - CkADADRecSheena Mae KitongNoch keine Bewertungen
- Appendix 34 - CkADADRecDokument1 SeiteAppendix 34 - CkADADRecMark Joseph BajaNoch keine Bewertungen
- Appendix 50 - PCFRec-2Dokument1 SeiteAppendix 50 - PCFRec-2Sherelyn MendozaNoch keine Bewertungen
- Appendix 50 - PCFRecDokument1 SeiteAppendix 50 - PCFRecRogie ApoloNoch keine Bewertungen