Das könnte Ihnen auch gefallen
- Genset Startup and Commissioning Checklist C 175Dokument3 SeitenGenset Startup and Commissioning Checklist C 175Dwi Mulyanti Dwimulyantishop100% (1)
- Dse890 Data SheetDokument4 SeitenDse890 Data Sheetdnps2011Noch keine Bewertungen
- 3.2 Powercommand 3.3 Spec Sheet S-1570Dokument11 Seiten3.2 Powercommand 3.3 Spec Sheet S-1570akheel201Noch keine Bewertungen
- Vm-10 (Diesel Generator Overhauling Report)Dokument1 SeiteVm-10 (Diesel Generator Overhauling Report)catalin67% (3)
- 6068HF158Dokument2 Seiten6068HF158Nabil Ibrahim100% (1)
- Operation and Maintenance Instructions Manual: Ju/Jw Model Engines FOR Fire Pump ApplicationsDokument38 SeitenOperation and Maintenance Instructions Manual: Ju/Jw Model Engines FOR Fire Pump ApplicationsangelvhNoch keine Bewertungen
- 4B3.3 Bolt TorquesDokument57 Seiten4B3.3 Bolt TorquesPanagiotis PanagosNoch keine Bewertungen
- Cat Compact Start Up and Commissioning ChecklistDokument19 SeitenCat Compact Start Up and Commissioning ChecklistAnonymous aufoLkcwhZ100% (1)
- Scheduling A Top End OverhaulDokument3 SeitenScheduling A Top End OverhaulVictor NunezNoch keine Bewertungen
- QSX15-G9 XpiDokument3 SeitenQSX15-G9 XpiMd ShNoch keine Bewertungen
- PDI ChecklistDokument2 SeitenPDI ChecklistAmmar Baig80% (5)
- Maintenance Standard Parts For 1 Unit Mitsubishi Engine S16R-PtaDokument6 SeitenMaintenance Standard Parts For 1 Unit Mitsubishi Engine S16R-Ptaali s100% (1)
- Caterpillar Genset Prime 400 EkW 500kvaDokument6 SeitenCaterpillar Genset Prime 400 EkW 500kvaYusuf Isman Wibowo100% (1)
- Crankcase Pressure SM019901095211 - en PDFDokument5 SeitenCrankcase Pressure SM019901095211 - en PDFDavy GonzalezNoch keine Bewertungen
- 7042 GL SpecDokument1 Seite7042 GL Specbkprice14Noch keine Bewertungen
- Daily Check ListDokument5 SeitenDaily Check Listarghyadeepjana100% (2)
- 1506a Operation and MaintenanceDokument112 Seiten1506a Operation and Maintenancemohammed mostafaNoch keine Bewertungen
- Specsheet 3516 1825 kVA PrimeDokument6 SeitenSpecsheet 3516 1825 kVA PrimeYusman EkaNoch keine Bewertungen
- QSK60 Over Head Valve Setting PerformaDokument2 SeitenQSK60 Over Head Valve Setting PerformaMuhammad Ishfaq100% (1)
- Cummins China 6LTAA8.9 G2Dokument5 SeitenCummins China 6LTAA8.9 G2nardjiNoch keine Bewertungen
- AKSA Diesel Generating Sets Installation Recommendations and Operations Manual-EnDokument64 SeitenAKSA Diesel Generating Sets Installation Recommendations and Operations Manual-EnWasinchai Kanjanapan100% (6)
- 6081HF001 EngineDokument2 Seiten6081HF001 EngineShahzad Ali100% (1)
- TWD1643 Service PartsDokument104 SeitenTWD1643 Service PartsDaniel Muratalla100% (1)
- Mainternal Interval 3406Dokument3 SeitenMainternal Interval 3406Sandy Sanjaya100% (1)
- K38 - Cylinder Head InstallationDokument3 SeitenK38 - Cylinder Head InstallationjengandxbNoch keine Bewertungen
- Job Card TemplateDokument2 SeitenJob Card TemplateAkash Rock43% (7)
- Operation and Maintenance Instructions Manual: Ju/Jw Model Engines FOR Fire Pump ApplicationsDokument53 SeitenOperation and Maintenance Instructions Manual: Ju/Jw Model Engines FOR Fire Pump ApplicationsJuan Castillo100% (2)
- Detroit Diesel Series 53 Service Manual 06Dokument69 SeitenDetroit Diesel Series 53 Service Manual 06tenbytwentytwo791067% (6)
- Perkins 1300 Series EdiDokument122 SeitenPerkins 1300 Series EdiFrederiko Molan100% (2)
- Cc200e h1 Cummins Mta11 G2a PDFDokument6 SeitenCc200e h1 Cummins Mta11 G2a PDFnaruto akatcyNoch keine Bewertungen
- Perkins Fault Finding GuideDokument13 SeitenPerkins Fault Finding GuideMksreekanthMk100% (2)
- SOP For 500kVA DG / Engine Fuel Pump Actuators & ECU Operating Conditions Checking / Failure AnalysisDokument22 SeitenSOP For 500kVA DG / Engine Fuel Pump Actuators & ECU Operating Conditions Checking / Failure AnalysisAaron VillareteNoch keine Bewertungen
- Manual Perkins 80kvaDokument4 SeitenManual Perkins 80kvaCristopher Alvial Muñoz100% (2)
- Maintenance Standard Parts For 1 Unit Mitsubishi Engine S16R-PtaDokument6 SeitenMaintenance Standard Parts For 1 Unit Mitsubishi Engine S16R-Ptaali sNoch keine Bewertungen
- Generator Monthly Check ListDokument1 SeiteGenerator Monthly Check Listsmart channelNoch keine Bewertungen
- Ems 927Dokument21 SeitenEms 927Er_raju100% (3)
- Generator - Test Sheet - UploadDokument3 SeitenGenerator - Test Sheet - Uploadchambigmac100% (2)
- Service Rutin 12 NHL 0296HJFDokument5 SeitenService Rutin 12 NHL 0296HJFAgung Adji WardanaNoch keine Bewertungen
- K 38Dokument1 SeiteK 38IKNoch keine Bewertungen
- Compressor: PDS175 (S) PDS655 (S)Dokument1 SeiteCompressor: PDS175 (S) PDS655 (S)Kamal SemboyNoch keine Bewertungen
- Cummins General Engine Data Sheet 6B, 6BT, 6BTADokument2 SeitenCummins General Engine Data Sheet 6B, 6BT, 6BTAMuebles Sanabria100% (1)
- Xq1475G Rental: Continuous 1475 KWDokument10 SeitenXq1475G Rental: Continuous 1475 KWEnerNoch keine Bewertungen
- Conectores Deutz - Cat Rehs0970Dokument104 SeitenConectores Deutz - Cat Rehs0970Miguel Angel Martinez DominguezNoch keine Bewertungen
- Cummins CatalogDokument88 SeitenCummins CatalogGazeto100% (2)
- Service Drawings Service Drawings: KTA38 Engine Platform KTA38 Engine PlatformDokument19 SeitenService Drawings Service Drawings: KTA38 Engine Platform KTA38 Engine PlatformKarim KadriNoch keine Bewertungen
- Operation and Maintenance Manual For Diesel Generator Sets: Everlasting CompanyDokument60 SeitenOperation and Maintenance Manual For Diesel Generator Sets: Everlasting CompanyYerson Manuel Aaron RoblesNoch keine Bewertungen
- Equipment History FormDokument3 SeitenEquipment History FormZwitsal Roslinda AuditorNoch keine Bewertungen
- Cummins Engine Overhaul - Service Scope ModfDokument3 SeitenCummins Engine Overhaul - Service Scope Modfjose favaNoch keine Bewertungen
- Fault Code: 2215 - SPN: 94 - FMI: 18: ISX CM871Dokument14 SeitenFault Code: 2215 - SPN: 94 - FMI: 18: ISX CM871Engr Ramez KaawachNoch keine Bewertungen
- WWW - Incar.tw-Cummins Vta28 Service ManualDokument5 SeitenWWW - Incar.tw-Cummins Vta28 Service ManualJhon Connor80% (5)
- Ues FSRDokument2 SeitenUes FSRFaisal ShahzadNoch keine Bewertungen
- I & C Check Sheet 717 F 14 2 Rev 02Dokument2 SeitenI & C Check Sheet 717 F 14 2 Rev 02winkyaw igtlNoch keine Bewertungen
- New Swift HB Owners Manual - 99011M55R00-74EDokument300 SeitenNew Swift HB Owners Manual - 99011M55R00-74ENox PlayerNoch keine Bewertungen
- At22 MaintenanceDokument37 SeitenAt22 MaintenancefabuleukalengaNoch keine Bewertungen
- Distribution Business Unit Cummins Field Service Report Pal Svam Power Solutions Private LTDDokument1 SeiteDistribution Business Unit Cummins Field Service Report Pal Svam Power Solutions Private LTDMalab TaufeekNoch keine Bewertungen
- Client: Project: Sheet 1 of 1 Date: Area: Pump Alignment ReportDokument8 SeitenClient: Project: Sheet 1 of 1 Date: Area: Pump Alignment ReportEky Aditya PutraNoch keine Bewertungen
- Pump Alignment Report FormatDokument3 SeitenPump Alignment Report Formatchua_jess86% (14)
- App HomeDokument3 SeitenApp HomesandyolkowskiNoch keine Bewertungen
- Tar 27Dokument4 SeitenTar 27ecoridembdNoch keine Bewertungen
- GeM Bidding 2936690Dokument5 SeitenGeM Bidding 2936690Sulvine CharlieNoch keine Bewertungen
- Osmania University, HyderabadDokument3 SeitenOsmania University, HyderabadNitesh K. YedatiNoch keine Bewertungen
- Welcome To WordDokument8 SeitenWelcome To WordMuhammad FajriNoch keine Bewertungen
- (A Govt. of India Enterprise Under The Ministry of Defence) : (Export Manufacturing Sbu - Bangalore Complex)Dokument6 Seiten(A Govt. of India Enterprise Under The Ministry of Defence) : (Export Manufacturing Sbu - Bangalore Complex)shuklaNoch keine Bewertungen
- Documentation CVDokument1 SeiteDocumentation CVNitesh K. YedatiNoch keine Bewertungen
- Add2-Exam RR Assistan 51Dokument1 SeiteAdd2-Exam RR Assistan 51Dhairya VyasNoch keine Bewertungen
- Operation Manual General-36R4XTDokument33 SeitenOperation Manual General-36R4XTMiguelNoch keine Bewertungen
- Gate 2015 S02Dokument24 SeitenGate 2015 S02Irfan ShaikhNoch keine Bewertungen
- Handbook On Level Crossing PDFDokument21 SeitenHandbook On Level Crossing PDFIztok Arshad100% (1)
- CL - Price List Dale Filter Systems Private Limited PDFDokument15 SeitenCL - Price List Dale Filter Systems Private Limited PDFBharti Puratan100% (1)
- Quantitative AptitudeDokument2 SeitenQuantitative AptitudeSivakumar MNoch keine Bewertungen
- Maximum Minimum Wage in Part I Part II Wef 01042015Dokument13 SeitenMaximum Minimum Wage in Part I Part II Wef 01042015Nitesh K. YedatiNoch keine Bewertungen
- Compact Concrete Batching PlantDokument8 SeitenCompact Concrete Batching PlantMunaNoch keine Bewertungen
- ME 1991 Unsolved PDFDokument13 SeitenME 1991 Unsolved PDFNitesh K. YedatiNoch keine Bewertungen
- ME 2012 Solved PDFDokument22 SeitenME 2012 Solved PDFNitesh K. YedatiNoch keine Bewertungen
- An Overview of Pharmaceutical ValidationDokument12 SeitenAn Overview of Pharmaceutical ValidationNarongchai PongpanNoch keine Bewertungen
- Stationary Concrete Pumps: For Highest Demands and Economical SolutionsDokument6 SeitenStationary Concrete Pumps: For Highest Demands and Economical SolutionsNitesh K. YedatiNoch keine Bewertungen
- Advt No 19 2017 EnglDokument47 SeitenAdvt No 19 2017 EnglSanjeev SahuNoch keine Bewertungen
- An Overview of Pharmaceutical ValidationDokument12 SeitenAn Overview of Pharmaceutical ValidationNarongchai PongpanNoch keine Bewertungen
- Revis 09Dokument24 SeitenRevis 09deekshithNoch keine Bewertungen
- Compact Concrete Batching PlantDokument8 SeitenCompact Concrete Batching PlantMunaNoch keine Bewertungen
- Compact Concrete Batching PlantDokument8 SeitenCompact Concrete Batching PlantMunaNoch keine Bewertungen
- Blake Mouton Managerial GridDokument3 SeitenBlake Mouton Managerial GridRashwanth Tc100% (1)
- بتول ماجد سعيد (تقرير السيطرة على تلوث الهواء)Dokument5 Seitenبتول ماجد سعيد (تقرير السيطرة على تلوث الهواء)Batool MagedNoch keine Bewertungen
- 53 English Work Book XDokument292 Seiten53 English Work Book XArun DhawanNoch keine Bewertungen
- AYUMJADokument1 SeiteAYUMJASoumet Das SoumetNoch keine Bewertungen
- English Test For Grade 7 (Term 2)Dokument6 SeitenEnglish Test For Grade 7 (Term 2)UyenPhuonggNoch keine Bewertungen
- Levels of CommunicationDokument3 SeitenLevels of CommunicationAiyaz ShaikhNoch keine Bewertungen
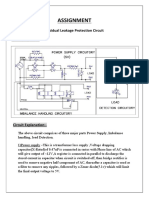
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDokument2 SeitenAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNoch keine Bewertungen
- PDS DeltaV SimulateDokument9 SeitenPDS DeltaV SimulateJesus JuarezNoch keine Bewertungen
- Audi A4-7Dokument532 SeitenAudi A4-7Anonymous QRVqOsa5Noch keine Bewertungen
- Strategic Management SlidesDokument150 SeitenStrategic Management SlidesIqra BilalNoch keine Bewertungen
- Civil Rights Vocabulary Lesson PlanDokument4 SeitenCivil Rights Vocabulary Lesson PlanKati ArmstrongNoch keine Bewertungen
- TTDM - JithinDokument24 SeitenTTDM - JithinAditya jainNoch keine Bewertungen
- Digital Systems Project: IITB CPUDokument7 SeitenDigital Systems Project: IITB CPUAnoushka DeyNoch keine Bewertungen
- Cameron International Corporation: FORM 10-KDokument31 SeitenCameron International Corporation: FORM 10-KMehdi SoltaniNoch keine Bewertungen
- Scrum Exam SampleDokument8 SeitenScrum Exam SampleUdhayaNoch keine Bewertungen
- Kübler 5800-5820 - enDokument5 SeitenKübler 5800-5820 - enpomsarexnbNoch keine Bewertungen
- Documentation Report On School's Direction SettingDokument24 SeitenDocumentation Report On School's Direction SettingSheila May FielNoch keine Bewertungen
- SSC Gr8 Biotech Q4 Module 1 WK 1 - v.01-CC-released-09May2021Dokument22 SeitenSSC Gr8 Biotech Q4 Module 1 WK 1 - v.01-CC-released-09May2021Ivy JeanneNoch keine Bewertungen
- Maximum and Minimum PDFDokument3 SeitenMaximum and Minimum PDFChai Usajai UsajaiNoch keine Bewertungen
- LG LFX31945 Refrigerator Service Manual MFL62188076 - Signature2 Brand DID PDFDokument95 SeitenLG LFX31945 Refrigerator Service Manual MFL62188076 - Signature2 Brand DID PDFplasmapete71% (7)
- Unit 1 PrinciplesDokument17 SeitenUnit 1 PrinciplesRohit YadavNoch keine Bewertungen
- Core CompetenciesDokument3 SeitenCore Competenciesapi-521620733Noch keine Bewertungen
- Installation 59TP6A 08SIDokument92 SeitenInstallation 59TP6A 08SIHenry SmithNoch keine Bewertungen
- Control ValvesDokument95 SeitenControl ValvesHardik Acharya100% (1)
- Sony x300 ManualDokument8 SeitenSony x300 ManualMarcosCanforaNoch keine Bewertungen
- Understanding The Contribution of HRM Bundles For Employee Outcomes Across The Life-SpanDokument15 SeitenUnderstanding The Contribution of HRM Bundles For Employee Outcomes Across The Life-SpanPhuong NgoNoch keine Bewertungen
- Bridge Over BrahmaputraDokument38 SeitenBridge Over BrahmaputraRahul DevNoch keine Bewertungen
- Anker Soundcore Mini, Super-Portable Bluetooth SpeakerDokument4 SeitenAnker Soundcore Mini, Super-Portable Bluetooth SpeakerM.SaadNoch keine Bewertungen
- Does Adding Salt To Water Makes It Boil FasterDokument1 SeiteDoes Adding Salt To Water Makes It Boil Fasterfelixcouture2007Noch keine Bewertungen
- SAMPLE MCQuestions ByTopicsDokument45 SeitenSAMPLE MCQuestions ByTopicsVeeru ManikantaNoch keine Bewertungen