Das könnte Ihnen auch gefallen
- DRUG SODIUM VALPROATE (Depakote, Epilim, Episenta)Dokument5 SeitenDRUG SODIUM VALPROATE (Depakote, Epilim, Episenta)Pearl Princess Guerrero100% (2)
- Objectives:: IndicationsDokument5 SeitenObjectives:: IndicationsChrisNoch keine Bewertungen
- Bab 22-23 Kaplan & Saddock Psychiatry Drug TreatmentDokument20 SeitenBab 22-23 Kaplan & Saddock Psychiatry Drug TreatmentCindy RaraNoch keine Bewertungen
- General: Genetic Implications: Pronunciation: Maz Trade Name(s)Dokument7 SeitenGeneral: Genetic Implications: Pronunciation: Maz Trade Name(s)jenm1228Noch keine Bewertungen
- AcetazolamideDokument4 SeitenAcetazolamideAnkit RuhilNoch keine Bewertungen
- Ativan CIV Tablets: R OnlyDokument8 SeitenAtivan CIV Tablets: R OnlyP KasikrishnarajaNoch keine Bewertungen
- ValiumDokument12 SeitenValiumAnonymous KPhTy0CENoch keine Bewertungen
- PharmacologyDokument116 SeitenPharmacologyvargheseNoch keine Bewertungen
- Drug Study OxbrytaDokument4 SeitenDrug Study OxbrytaCatherine PradoNoch keine Bewertungen
- DrugDokument13 SeitenDrugkhesler BacallaNoch keine Bewertungen
- Valproic AcidDokument4 SeitenValproic Acidapi-3797941100% (2)
- Metronidazole: IntravenousDokument4 SeitenMetronidazole: IntravenousShiela May GoNoch keine Bewertungen
- Pharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityDokument37 SeitenPharmacology of CNS: Prajogo Wibowo Faculty of Medicine Hang Tuah UniversityIda Bagus Putu SwabawaNoch keine Bewertungen
- Valproic AcidDokument4 SeitenValproic AcidAndrea Huecas TriaNoch keine Bewertungen
- Carboxylic Acid DerivativesDokument3 SeitenCarboxylic Acid Derivativesshai padillaNoch keine Bewertungen
- 33-36 Medications PDFDokument15 Seiten33-36 Medications PDFJeraldine GumpalNoch keine Bewertungen
- ImipramineDokument6 SeitenImipramineMuhammed Faruk JambazNoch keine Bewertungen
- Geriatrics Department BookDokument69 SeitenGeriatrics Department BookHazemAbu-BakrNoch keine Bewertungen
- CLobazamDokument7 SeitenCLobazamnika0126Noch keine Bewertungen
- GENERIC NAME: Omeprazole, Omeprazole/sodium BicarbonateDokument4 SeitenGENERIC NAME: Omeprazole, Omeprazole/sodium BicarbonateKnowell CadienteNoch keine Bewertungen
- AripiprazoleDokument4 SeitenAripiprazoleAP TOROBX100% (1)
- Sodium ValproateDokument15 SeitenSodium ValproatedrdeuceNoch keine Bewertungen
- CarbamazepineDokument5 SeitenCarbamazepineapi-3797941100% (2)
- Drug StudyDokument8 SeitenDrug StudyLea FestejoNoch keine Bewertungen
- Nursing Diagnosing (PDAR)Dokument4 SeitenNursing Diagnosing (PDAR)dakieNoch keine Bewertungen
- 24 0 PDFDokument12 Seiten24 0 PDFAna-Mihaela BalanutaNoch keine Bewertungen
- DrugsDokument8 SeitenDrugsShizuka Marycris AmaneNoch keine Bewertungen
- Effexor Package InsertDokument53 SeitenEffexor Package InsertpatgarettNoch keine Bewertungen
- Drug Prescription in CKD and DialysisDokument24 SeitenDrug Prescription in CKD and DialysisAnitha SNoch keine Bewertungen
- Diuretics: Generic Name: FUROSEMIDEDokument12 SeitenDiuretics: Generic Name: FUROSEMIDEJR BetonioNoch keine Bewertungen
- Qlaira en PiDokument10 SeitenQlaira en PidrclaudiofernandomedNoch keine Bewertungen
- C C C CC C MMMM MMMMDokument10 SeitenC C C CC C MMMM MMMMFerlyn PanchoNoch keine Bewertungen
- LevetiracetamDokument3 SeitenLevetiracetamSanny KajarNoch keine Bewertungen
- Dipyrone (Metamizole) : Pronunciation Brand Names: InternationalDokument9 SeitenDipyrone (Metamizole) : Pronunciation Brand Names: InternationalRismaya AminiNoch keine Bewertungen
- 02 JJJKK 51 S 051 LBLDokument21 Seiten02 JJJKK 51 S 051 LBLSofiNoch keine Bewertungen
- Vesanoid (Tretinoin) Capsules R Only Warnings 1. Experienced Physician and InstitutionDokument14 SeitenVesanoid (Tretinoin) Capsules R Only Warnings 1. Experienced Physician and InstitutionArun GargNoch keine Bewertungen
- Data Sheet: VesicareDokument10 SeitenData Sheet: VesicareumarNoch keine Bewertungen
- Voltfast-Sep 2022.SIN-app260123 PDFDokument14 SeitenVoltfast-Sep 2022.SIN-app260123 PDFChelang AbdulkareemNoch keine Bewertungen
- Regulatory Document2 EngDokument201 SeitenRegulatory Document2 EngDomenico LombardiniNoch keine Bewertungen
- Outline Drug Therapy in Older AdultsDokument4 SeitenOutline Drug Therapy in Older Adultsswillis1Noch keine Bewertungen
- ValdoxanDokument27 SeitenValdoxanPetre FallNoch keine Bewertungen
- EsomeprazoleDokument1 SeiteEsomeprazoleamaliea234Noch keine Bewertungen
- To Pi Ram AteDokument3 SeitenTo Pi Ram Ateapi-3797941Noch keine Bewertungen
- Chlorpromazine Drug StudyDokument7 SeitenChlorpromazine Drug Studyjennachristy03100% (3)
- Valproate SodiumDokument2 SeitenValproate SodiumKhairul KhairulNoch keine Bewertungen
- Valproic Acid Poisoning - UpToDateDokument25 SeitenValproic Acid Poisoning - UpToDateLaura VargasNoch keine Bewertungen
- Omeprazole: Losec 40 MG Powder and Solvent For Solution For Injection CompositionDokument11 SeitenOmeprazole: Losec 40 MG Powder and Solvent For Solution For Injection CompositionNadia AfifahNoch keine Bewertungen
- Ospolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)Dokument7 SeitenOspolot 200 MG, Film-Coated Tablets: Summary of Product Characteristics (SPC)ddandan_2Noch keine Bewertungen
- Mefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysiaDokument1 SeiteMefenamic Acid Indication, Dosage, Side Effect, Precaution MIMS MalaysianuruladyanisaifuzzamanNoch keine Bewertungen
- Theselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsDokument10 SeitenTheselectionof Antiepilepticdrugs Forthetreatmentof Epilepsyinchildren AndadultsFaizan MazharNoch keine Bewertungen
- PI DuphalacDokument2 SeitenPI Duphalacabin prakashNoch keine Bewertungen
- PREVPAC Drug StudyDokument7 SeitenPREVPAC Drug StudyAngela ReyesNoch keine Bewertungen
- Ospolot Sulthiame 50 MG - 200 MG Tablet PI V08 DT 21 Nov 2013Dokument5 SeitenOspolot Sulthiame 50 MG - 200 MG Tablet PI V08 DT 21 Nov 2013iuliamzaNoch keine Bewertungen
- ATIVAN (Lorazepam) Injection, USPDokument20 SeitenATIVAN (Lorazepam) Injection, USPsanthoshNoch keine Bewertungen
- Availability: Verapamil HydrochlorideDokument21 SeitenAvailability: Verapamil Hydrochloridesteffy sojanNoch keine Bewertungen
- Clozapine (Drug Study)Dokument2 SeitenClozapine (Drug Study)Franz.thenurse6888100% (3)
- Eti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaDokument43 SeitenEti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaadystiNoch keine Bewertungen
- Drug Prescribing in Renal Impairment Information. Patient PatientDokument13 SeitenDrug Prescribing in Renal Impairment Information. Patient PatientEffy AngeLi LomocsoNoch keine Bewertungen
- Anti-Seizure Medications: by Dawit S. (R3)Dokument53 SeitenAnti-Seizure Medications: by Dawit S. (R3)ጉራማይሌ TubeNoch keine Bewertungen
- Insert INFUSAN D5 + NSDokument2 SeitenInsert INFUSAN D5 + NSNurul HusnaNoch keine Bewertungen
- Banned DrugsDokument3 SeitenBanned Drugsmanvitha varmaNoch keine Bewertungen
- FDA's Current Practice and Challenges in The Use of Dissolution Similarity Testing For Demonstration of Bioequivalence - Case StudiesDokument19 SeitenFDA's Current Practice and Challenges in The Use of Dissolution Similarity Testing For Demonstration of Bioequivalence - Case StudiesSrinivas Reddy MaramNoch keine Bewertungen
- Form Laporan Pustu PonkesdesDokument10 SeitenForm Laporan Pustu PonkesdesoctieNoch keine Bewertungen
- Skin Grafting SurgeryDokument15 SeitenSkin Grafting SurgeryVithikaNoch keine Bewertungen
- Formulation Design, Challenges, and Development Considerations For Fixed Dose Combination (FDC) of Oral Solid Dosage FormsDokument13 SeitenFormulation Design, Challenges, and Development Considerations For Fixed Dose Combination (FDC) of Oral Solid Dosage FormsirasafitriNoch keine Bewertungen
- Antihypertensive DrugsDokument5 SeitenAntihypertensive DrugsAiman TymerNoch keine Bewertungen
- The Art of Counselling and Psychotherapy: January 2004Dokument2 SeitenThe Art of Counselling and Psychotherapy: January 2004Shanica Paul-RichardsNoch keine Bewertungen
- DAFTAR PENERIMAAN (Version 1)Dokument342 SeitenDAFTAR PENERIMAAN (Version 1)fennyrahmaNoch keine Bewertungen
- Prescription Job AidsDokument16 SeitenPrescription Job AidsbakaNoch keine Bewertungen
- Emergency Drugs: Drug Classification USE Stock Dose Nursing ConsiderationDokument4 SeitenEmergency Drugs: Drug Classification USE Stock Dose Nursing Considerationrhennifer100% (1)
- Seizures and Epilepsy in Patients With Ischaemic StrokeDokument17 SeitenSeizures and Epilepsy in Patients With Ischaemic StrokeAnali Durán CorderoNoch keine Bewertungen
- Duke University Nurse Anesthesia Program (Acct #7042) Montgomery, Kelly Barton (Semester 7) Is Logged inDokument3 SeitenDuke University Nurse Anesthesia Program (Acct #7042) Montgomery, Kelly Barton (Semester 7) Is Logged inkellyb11Noch keine Bewertungen
- 68 - What Is Kratom 20 Jul 2020Dokument3 Seiten68 - What Is Kratom 20 Jul 2020Rizal DaudNoch keine Bewertungen
- Module 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHDokument135 SeitenModule 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHJojo DelosreyesNoch keine Bewertungen
- Emergency TreatmentDokument5 SeitenEmergency TreatmentAdina IqbalNoch keine Bewertungen
- Enhanced Recovery ProtocolsDokument17 SeitenEnhanced Recovery ProtocolsHening Tirta KusumawardaniNoch keine Bewertungen
- Handy Chart DepressionDokument2 SeitenHandy Chart DepressionsteadiNoch keine Bewertungen
- Drug Approval System in MalaysiaDokument47 SeitenDrug Approval System in MalaysiaAnu PariyarathNoch keine Bewertungen
- Medic Nes Control Authority of ZimbabweDokument2 SeitenMedic Nes Control Authority of ZimbabweMunyanduki TapiwaNoch keine Bewertungen
- Meglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andDokument6 SeitenMeglitinide Analogues Are Classified As Insulin Secretagogues and Have Actions andRifqoh Aulia AlthofunnisaNoch keine Bewertungen
- Drug Study - Cholopromazine DivalDokument3 SeitenDrug Study - Cholopromazine Divalgoody1286Noch keine Bewertungen
- PaclitaxelDokument4 SeitenPaclitaxelAdditi SatyalNoch keine Bewertungen
- Achieving Market Dominance Through ReformulationDokument223 SeitenAchieving Market Dominance Through ReformulationHerry HendrayadiNoch keine Bewertungen
- Introduction To PharmacologyDokument11 SeitenIntroduction To PharmacologyMaryam ElammaryNoch keine Bewertungen
- Pharmaco TherapeuticsDokument19 SeitenPharmaco TherapeuticsJareena BegumNoch keine Bewertungen
- Antibiotic Cross-Sensitivity ChartDokument1 SeiteAntibiotic Cross-Sensitivity ChartChing JuNoch keine Bewertungen
- Pharmacology BookDokument332 SeitenPharmacology BookKenneth DayritNoch keine Bewertungen
- Set Rec Pic 829Dokument2 SeitenSet Rec Pic 829Peter SalimNoch keine Bewertungen
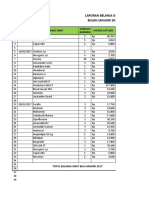
- Laporan Belanja Obat Bulan Januari 2017: No Tanggal Nama Obat Harga Satuan Jumlah BarangDokument16 SeitenLaporan Belanja Obat Bulan Januari 2017: No Tanggal Nama Obat Harga Satuan Jumlah Barangcitra husadaNoch keine Bewertungen