Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hotel Manuals Sop - Kitchen PDFDokument66 SeitenHotel Manuals Sop - Kitchen PDFsetiawan100% (3)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- F & B Production Lesson 1Dokument64 SeitenF & B Production Lesson 1jkimamoNoch keine Bewertungen
- How Important Is Vitamin D For Your Health? Let Us Count The Ways ...Dokument8 SeitenHow Important Is Vitamin D For Your Health? Let Us Count The Ways ...Homework PingNoch keine Bewertungen
- In Vivo Relevance For Photo Protection by The Vitamin D Rapid Response Pathway 2007Dokument6 SeitenIn Vivo Relevance For Photo Protection by The Vitamin D Rapid Response Pathway 2007ytreffalNoch keine Bewertungen
- Fracture Prevention With Vitamin D Supplementation. REVIEW. Bischoff-Ferrari, Et Al., 2005.Dokument8 SeitenFracture Prevention With Vitamin D Supplementation. REVIEW. Bischoff-Ferrari, Et Al., 2005.ytreffalNoch keine Bewertungen
- Identification of Novel Mediators of Vitamin D Signaling and 1,25 (OH) 2D3 Resistance in Mammary CellsDokument5 SeitenIdentification of Novel Mediators of Vitamin D Signaling and 1,25 (OH) 2D3 Resistance in Mammary CellsytreffalNoch keine Bewertungen
- Vitamin d10 2Dokument18 SeitenVitamin d10 2willianmeNoch keine Bewertungen
- Inhibition of Prostate Growth and Inflammation by The Vitamin D Receptor Agonist BXL-628 ElocalcitolDokument5 SeitenInhibition of Prostate Growth and Inflammation by The Vitamin D Receptor Agonist BXL-628 ElocalcitolytreffalNoch keine Bewertungen
- Vitamin D An Old Vitamin With New Health Implications (PDF 208k)Dokument4 SeitenVitamin D An Old Vitamin With New Health Implications (PDF 208k)ytreffalNoch keine Bewertungen
- Fact Sheet On Vitamin DDokument11 SeitenFact Sheet On Vitamin DKerri Knox100% (4)
- D Vitamin D - More Than A Bone-a-Fide HormoneDokument15 SeitenD Vitamin D - More Than A Bone-a-Fide Hormoneytreffal100% (1)
- 2 - D Vitamin D Insufficiency in North America (PDF) HANLEYDokument6 Seiten2 - D Vitamin D Insufficiency in North America (PDF) HANLEYytreffalNoch keine Bewertungen
- Dietary Recommendations For Vitamin D Need To Establish An Estimated Average Requirement. Whiting, and CalvoDokument6 SeitenDietary Recommendations For Vitamin D Need To Establish An Estimated Average Requirement. Whiting, and CalvoytreffalNoch keine Bewertungen
- D Vitamin D Insufficiency - No Recommended Dietary Allowance Exists For This Nutrient COMMENTARY-VIETH, FRASER 11JUN02Dokument2 SeitenD Vitamin D Insufficiency - No Recommended Dietary Allowance Exists For This Nutrient COMMENTARY-VIETH, FRASER 11JUN02ytreffalNoch keine Bewertungen
- Dietary Intake of Vitamins B6, B12 and Folate in Relation To Homocysteine Serum Concentration, Dietary, 2010Dokument8 SeitenDietary Intake of Vitamins B6, B12 and Folate in Relation To Homocysteine Serum Concentration, Dietary, 2010ytreffalNoch keine Bewertungen
- Calcium and Vitamin D (Tropicana Fact Sheet) ADA FACT SHEETDokument2 SeitenCalcium and Vitamin D (Tropicana Fact Sheet) ADA FACT SHEETytreffalNoch keine Bewertungen
- Fracture Prevention With Vitamin D Supplementation. REVIEW. Bischoff-Ferrari, Et Al., 2005.Dokument8 SeitenFracture Prevention With Vitamin D Supplementation. REVIEW. Bischoff-Ferrari, Et Al., 2005.ytreffalNoch keine Bewertungen
- D Symposium - Vitamin D Insufficiency - CALVO, WHITINGDokument3 SeitenD Symposium - Vitamin D Insufficiency - CALVO, WHITINGytreffalNoch keine Bewertungen
- Identification of Novel Mediators of Vitamin D Signaling and 1,25 (OH) 2D3 Resistance in Mammary CellsDokument5 SeitenIdentification of Novel Mediators of Vitamin D Signaling and 1,25 (OH) 2D3 Resistance in Mammary CellsytreffalNoch keine Bewertungen
- High-Dose Vitamin Therapy Stimulates Variant Enzymes With Decreased Coenzyme Binding AffinityDokument43 SeitenHigh-Dose Vitamin Therapy Stimulates Variant Enzymes With Decreased Coenzyme Binding AffinityytreffalNoch keine Bewertungen
- Association of Low Intake of Milk and Vitamin D During Pregnancy With Decreased Birth Weight. Mannion, Gray-Donald, Koski. 2006Dokument5 SeitenAssociation of Low Intake of Milk and Vitamin D During Pregnancy With Decreased Birth Weight. Mannion, Gray-Donald, Koski. 2006ytreffalNoch keine Bewertungen
- Vitamin d10 2Dokument18 SeitenVitamin d10 2willianmeNoch keine Bewertungen
- High Prevalence of Vitamin D Deficiency in Pregnant Non-Western Women in The Hague, Netherlands. Van Der Meer, Et Al., 2006.Dokument4 SeitenHigh Prevalence of Vitamin D Deficiency in Pregnant Non-Western Women in The Hague, Netherlands. Van Der Meer, Et Al., 2006.ytreffalNoch keine Bewertungen
- Dietary Recommendations For Vitamin D Need To Establish An Estimated Average Requirement. Whiting, and CalvoDokument6 SeitenDietary Recommendations For Vitamin D Need To Establish An Estimated Average Requirement. Whiting, and CalvoytreffalNoch keine Bewertungen
- Gamma-Tocopherol or Combinations of Vitamin E Forms Induce Cell Death in Human Prostate Cancer Cells. Jiang, Et Al., 2004.Dokument6 SeitenGamma-Tocopherol or Combinations of Vitamin E Forms Induce Cell Death in Human Prostate Cancer Cells. Jiang, Et Al., 2004.ytreffalNoch keine Bewertungen
- Vitamin d10 2Dokument18 SeitenVitamin d10 2willianmeNoch keine Bewertungen
- 6 - Vitamin D Requirements - Current and Future. WEAVER, FLEET AJCN DEC04Dokument5 Seiten6 - Vitamin D Requirements - Current and Future. WEAVER, FLEET AJCN DEC04ytreffalNoch keine Bewertungen
- 4 - Racial-Ethnic Vitamin D For Adult and Elderly Men and WomDokument4 Seiten4 - Racial-Ethnic Vitamin D For Adult and Elderly Men and WomytreffalNoch keine Bewertungen
- 13th Workshop Consensus For Vitamin D Nutritional Guidelines JSB& MB 103 (2007) 204-205Dokument2 Seiten13th Workshop Consensus For Vitamin D Nutritional Guidelines JSB& MB 103 (2007) 204-205ytreffalNoch keine Bewertungen
- A Call For More Vitamin D Research PDFDokument3 SeitenA Call For More Vitamin D Research PDFytreffalNoch keine Bewertungen
- 6 - Vitamin D Requirements - Current and Future. WEAVER, FLEET AJCN DEC04Dokument5 Seiten6 - Vitamin D Requirements - Current and Future. WEAVER, FLEET AJCN DEC04ytreffalNoch keine Bewertungen
- 4 - Racial-Ethnic Vitamin D For Adult and Elderly Men and WomDokument4 Seiten4 - Racial-Ethnic Vitamin D For Adult and Elderly Men and WomytreffalNoch keine Bewertungen
- Codex One Page FlyerDokument1 SeiteCodex One Page Flyerstopcodex100% (2)
- Notice: Reports and Guidance Documents Availability, Etc.: Bovine Spongiform Encephalopathy Harvard Risk Assessment Update Technical MeetingDokument2 SeitenNotice: Reports and Guidance Documents Availability, Etc.: Bovine Spongiform Encephalopathy Harvard Risk Assessment Update Technical MeetingJustia.comNoch keine Bewertungen
- SCCP - o - 03j (Full)Dokument106 SeitenSCCP - o - 03j (Full)Uwe GreulachNoch keine Bewertungen
- 18 - PH Measurement in The Acidification Process of Fermented SausagesDokument2 Seiten18 - PH Measurement in The Acidification Process of Fermented SausagesDavid Suarez Chacon100% (1)
- N PM A Food Safety Audit Scheme Reference GuideDokument5 SeitenN PM A Food Safety Audit Scheme Reference GuideOscar Fernando Serrano Fuentes0% (1)
- Food IrradiationDokument15 SeitenFood IrradiationVivek KumarNoch keine Bewertungen
- Unit 208 Understand Health and Safety in Social Care SettingDokument8 SeitenUnit 208 Understand Health and Safety in Social Care Settingamacovei_375% (4)
- Mikrobiologi MakananDokument30 SeitenMikrobiologi MakananmuhdakmalNoch keine Bewertungen
- Beer ProceassDokument251 SeitenBeer ProceassAjay Tiwari100% (1)
- Different Types of Smokehouses and Smokehouse PlansDokument5 SeitenDifferent Types of Smokehouses and Smokehouse PlansEloisa OleaNoch keine Bewertungen
- Deepak Memorialacademy School: Study of Effect of Potassium Bisulphite As A Food PreservativeDokument25 SeitenDeepak Memorialacademy School: Study of Effect of Potassium Bisulphite As A Food PreservativeRehan AhmadNoch keine Bewertungen
- Annotated BibliographyDokument2 SeitenAnnotated Bibliographyapi-2606319570% (1)
- FDADokument27 SeitenFDArahul364Noch keine Bewertungen
- Visit To Pakistan: John Osullivan Zheng BeibeiDokument5 SeitenVisit To Pakistan: John Osullivan Zheng Beibeinaeem186Noch keine Bewertungen
- Intermediate Moisture FoodsDokument12 SeitenIntermediate Moisture FoodsRohit Sandilya50% (2)
- What Is Mental Health or Emotional HealthDokument5 SeitenWhat Is Mental Health or Emotional HealthAl LanNoch keine Bewertungen
- Checklist Auditoria SQF 2010Dokument21 SeitenChecklist Auditoria SQF 2010cramirez48Noch keine Bewertungen
- Third-Party Audit AgenciesDokument12 SeitenThird-Party Audit AgenciesRAMESHNoch keine Bewertungen
- HACCP PrinciplesDokument2 SeitenHACCP PrinciplesnisbabaNoch keine Bewertungen
- Health Warning On Diwa Grated Coconut Which May Be Contaminated With SalmonellaDokument2 SeitenHealth Warning On Diwa Grated Coconut Which May Be Contaminated With SalmonellaPiPharmNoch keine Bewertungen
- FG FICQ0103 Jam Jelly and Ketchup Processing Technician 15-12-2017Dokument224 SeitenFG FICQ0103 Jam Jelly and Ketchup Processing Technician 15-12-2017Leila Espinosa100% (1)
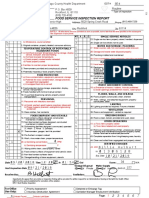
- Winnebago County Health Department, Food Service Inspection Report, Guilford High SchoolDokument7 SeitenWinnebago County Health Department, Food Service Inspection Report, Guilford High Schoolcorina curryNoch keine Bewertungen
- Hygienic Design of Food Industry EquipmentDokument10 SeitenHygienic Design of Food Industry EquipmentBồ Công AnhNoch keine Bewertungen
- Food Additives and PreservativesDokument5 SeitenFood Additives and PreservativesNur Adibah JalaluddinNoch keine Bewertungen
- Food Safety Plan of Catalonia: GuidelinesDokument38 SeitenFood Safety Plan of Catalonia: GuidelinesralapubsNoch keine Bewertungen
- Food DehydratorDokument54 SeitenFood DehydratorSusan Anderson100% (2)
- Food Safety in IndiaDokument37 SeitenFood Safety in IndiariddhisanghviNoch keine Bewertungen
- Canteen Policy Support DocumentDokument8 SeitenCanteen Policy Support DocumentKeneth Del CarmenNoch keine Bewertungen