Das könnte Ihnen auch gefallen
- Vadim Moskvin 2002 Phys. Med. Biol. 47 301Dokument18 SeitenVadim Moskvin 2002 Phys. Med. Biol. 47 301SUBHANoch keine Bewertungen
- Investigation of Physical Penumbra Definition inDokument6 SeitenInvestigation of Physical Penumbra Definition indumitracheNoch keine Bewertungen
- Radiation Measurements: J.L. Vega Ramirez, F. Chen, P. Nicolucci, O. BaffaDokument4 SeitenRadiation Measurements: J.L. Vega Ramirez, F. Chen, P. Nicolucci, O. BaffaZeka ValladolidNoch keine Bewertungen
- Sequence Optimization For MRI Acoustic NoiseDokument9 SeitenSequence Optimization For MRI Acoustic NoiseArsy ZygomaticNoch keine Bewertungen
- Physics Today-June 2021Dokument73 SeitenPhysics Today-June 2021Gavril BogdanNoch keine Bewertungen
- Metaxas 2015 J. Phys.: Conf. Ser. 637 012017Dokument5 SeitenMetaxas 2015 J. Phys.: Conf. Ser. 637 012017Lani DianaNoch keine Bewertungen
- W Xiong 2007 J. Phys. Conf. Ser. 74 021023Dokument11 SeitenW Xiong 2007 J. Phys. Conf. Ser. 74 021023SUBHANoch keine Bewertungen
- IMRT: A Review and Preview: Physics in Medicine & BiologyDokument18 SeitenIMRT: A Review and Preview: Physics in Medicine & BiologychatsashNoch keine Bewertungen
- Dermal fibroblast infiltration of poly (ε-caprolactone) scaffolds fabricated by melt electrospinning in a direct writing modeDokument12 SeitenDermal fibroblast infiltration of poly (ε-caprolactone) scaffolds fabricated by melt electrospinning in a direct writing modeMelanie FerraceNoch keine Bewertungen
- Biosensors and Bioelectronics: A B A ADokument7 SeitenBiosensors and Bioelectronics: A B A AALEJANDRA JIMENEZNoch keine Bewertungen
- Study of Langmuir Monolayers and Langmuir-SchaeferDokument7 SeitenStudy of Langmuir Monolayers and Langmuir-SchaeferAmar AmarNoch keine Bewertungen
- Applicationofimaging Technologiesinthe InvestigationofdrugaddictionDokument16 SeitenApplicationofimaging Technologiesinthe Investigationofdrugaddictionstein godoy pachecoNoch keine Bewertungen
- Probing supersymmetric leptogenesis with μ→ eγ: Journal of High Energy PhysicsDokument22 SeitenProbing supersymmetric leptogenesis with μ→ eγ: Journal of High Energy Physicscifarha venantNoch keine Bewertungen
- Journal FizikDokument8 SeitenJournal FizikSiti NadhirahNoch keine Bewertungen
- Verification of Dosimetric Materials To Be Used As Tissue-SubstitutesDokument11 SeitenVerification of Dosimetric Materials To Be Used As Tissue-SubstitutesMauricio L GomezNoch keine Bewertungen
- Mohammed 2016Dokument9 SeitenMohammed 2016A DNoch keine Bewertungen
- MRI MohemDokument7 SeitenMRI Mohema.mahdieh90Noch keine Bewertungen
- Brambilla 2005Dokument8 SeitenBrambilla 2005shahhareshNoch keine Bewertungen
- Jana 03Dokument5 SeitenJana 03Dr. Amit Kumar JanaNoch keine Bewertungen
- Borodovsky Bioinformatics 2001 PDFDokument3 SeitenBorodovsky Bioinformatics 2001 PDFNaura CorporationNoch keine Bewertungen
- Human Brain Mapping - 2020 - Cruz - Interrelations Between Dopamine and Serotonin Producing Sites and Regions of The PDFDokument13 SeitenHuman Brain Mapping - 2020 - Cruz - Interrelations Between Dopamine and Serotonin Producing Sites and Regions of The PDFWynn TheinNoch keine Bewertungen
- 3dprinted Scaffolds Based On PLAHA Nanocomposites For Trabecular Bone Reconstructionjournal of Physics Conference SeriesDokument6 Seiten3dprinted Scaffolds Based On PLAHA Nanocomposites For Trabecular Bone Reconstructionjournal of Physics Conference Seriesrafael asssuncaoNoch keine Bewertungen
- Evidence For EMF Transcriptomics and Proteomics Research 2007-2012Dokument41 SeitenEvidence For EMF Transcriptomics and Proteomics Research 2007-2012YooHinomuraNoch keine Bewertungen
- Lazebnik 2005 Phys. Med. Biol. 50 4245 PDFDokument15 SeitenLazebnik 2005 Phys. Med. Biol. 50 4245 PDFUğur Berkay ÇalışkanNoch keine Bewertungen
- Effective Dose Conversion Coefficients CalculatedDokument11 SeitenEffective Dose Conversion Coefficients CalculatedtatamaxNoch keine Bewertungen
- Pappas 2017 Phys. Med. Biol. 62 4160Dokument24 SeitenPappas 2017 Phys. Med. Biol. 62 4160SUBHANoch keine Bewertungen
- Principles of Electrical Impedance Tomography and Its Clinical ApplicationDokument12 SeitenPrinciples of Electrical Impedance Tomography and Its Clinical ApplicationЕгор КазанцевNoch keine Bewertungen
- Prognostics of PEM Fuel Cell in A ParticDokument12 SeitenPrognostics of PEM Fuel Cell in A ParticJairo Castro FlorianNoch keine Bewertungen
- Alagapan JNeuralEng 2019Dokument13 SeitenAlagapan JNeuralEng 2019oswalt.dnNoch keine Bewertungen
- Tange Stan I 2001Dokument8 SeitenTange Stan I 2001ابوبكر عبد الباقيNoch keine Bewertungen
- Analysis of Apparent 1 - F - Alpha Spectrum in DNA Sequences.B. - Borstnik - 1993 - EPL - 23 - 002Dokument7 SeitenAnalysis of Apparent 1 - F - Alpha Spectrum in DNA Sequences.B. - Borstnik - 1993 - EPL - 23 - 002Yttria TherbiumNoch keine Bewertungen
- Lampe 2018Dokument11 SeitenLampe 2018Chloe FanningNoch keine Bewertungen
- Fabian I 2007Dokument3 SeitenFabian I 2007meripe sureshNoch keine Bewertungen
- 1Dokument11 Seiten1putriNoch keine Bewertungen
- Methods: Construction of A Workflow For Genome-Wide Variation Analysis of Formalin Fixed Paraffin Embedded Tumor SamplesDokument1 SeiteMethods: Construction of A Workflow For Genome-Wide Variation Analysis of Formalin Fixed Paraffin Embedded Tumor SamplesZelha NilNoch keine Bewertungen
- Esplen 2022 Phys. Med. Biol. 67 105003Dokument25 SeitenEsplen 2022 Phys. Med. Biol. 67 105003souhaila soulNoch keine Bewertungen
- 2013 Nanoparticle Decoration of CNTs by Sputtering CarbonDokument9 Seiten2013 Nanoparticle Decoration of CNTs by Sputtering CarbonMrudulaNoch keine Bewertungen
- 3D Dose Computation AlgorithmsDokument10 Seiten3D Dose Computation AlgorithmsHashir SaeedNoch keine Bewertungen
- Hoff 2017Dokument1 SeiteHoff 2017Saadia BenhaloucheNoch keine Bewertungen
- Acsami 0c13865Dokument12 SeitenAcsami 0c13865dwid jansNoch keine Bewertungen
- Recent Advances in Biomagnetism and Its ApplicationsDokument2 SeitenRecent Advances in Biomagnetism and Its ApplicationsnoiodaNoch keine Bewertungen
- 1 s2.0 S0892199721001879 MainDokument8 Seiten1 s2.0 S0892199721001879 MainAbdelkbir WsNoch keine Bewertungen
- Fleming 2021 J. Neural Eng. 18 041004Dokument23 SeitenFleming 2021 J. Neural Eng. 18 041004u5600291Noch keine Bewertungen
- Ijn 7 2863Dokument10 SeitenIjn 7 2863a.mahdieh90Noch keine Bewertungen
- Time-Frequency Analysis of Non-Stationary Signals in Fusion Plasmas Using The Choi-Williams DistributionDokument5 SeitenTime-Frequency Analysis of Non-Stationary Signals in Fusion Plasmas Using The Choi-Williams DistributionJaya KumarNoch keine Bewertungen
- Signal-To-Noise Ratio Evaluation in ResonantDokument13 SeitenSignal-To-Noise Ratio Evaluation in ResonantFabian VazquezNoch keine Bewertungen
- A Point Kernel Algorithm For Microbeam Radiation Therapy: Physics in Medicine & BiologyDokument20 SeitenA Point Kernel Algorithm For Microbeam Radiation Therapy: Physics in Medicine & BiologyPiotr JankowskiNoch keine Bewertungen
- Maffini 2017 Nucl. Fusion 57 046014Dokument14 SeitenMaffini 2017 Nucl. Fusion 57 046014Nord KappNoch keine Bewertungen
- SEM - FIB Imaging For Studying Neural InterfacesDokument11 SeitenSEM - FIB Imaging For Studying Neural InterfacesUNIG Aluana SantanaNoch keine Bewertungen
- Pigment Cell & Melanoma Research: DOI: 10.1111/pcmr.12535Dokument7 SeitenPigment Cell & Melanoma Research: DOI: 10.1111/pcmr.12535dwyphyNoch keine Bewertungen
- Validation of The GEANT4 Simulation of BremsstrahlDokument16 SeitenValidation of The GEANT4 Simulation of Bremsstrahlsouhaila soulNoch keine Bewertungen
- ml-0538 HaptotaxisDokument2 Seitenml-0538 Haptotaxisapi-457366236Noch keine Bewertungen
- Effect of Filter On Average Glandular Dose and Image Quality in Digital MammographyDokument6 SeitenEffect of Filter On Average Glandular Dose and Image Quality in Digital MammographyEsteban PalaciosNoch keine Bewertungen
- Eb2 NiwDokument5 SeitenEb2 NiwAhmad EsmaeilkhahNoch keine Bewertungen
- Ref 2Dokument13 SeitenRef 2Chit Su HlaingNoch keine Bewertungen
- 2 Reyes-Gómez - 2009 - EPL - 88 - 24002Dokument7 Seiten2 Reyes-Gómez - 2009 - EPL - 88 - 24002Jaime David Díaz RamírezNoch keine Bewertungen
- ESAO2014 CaniDokument2 SeitenESAO2014 CaniElisabetta ZanettiNoch keine Bewertungen
- Endothelium: Please Scroll Down For ArticleDokument12 SeitenEndothelium: Please Scroll Down For Articleshimonl3892Noch keine Bewertungen
- Cita 2 11751302Dokument12 SeitenCita 2 11751302Tetrahedro AndrésNoch keine Bewertungen
- V Evs QBDokument7 SeitenV Evs QBSUBHANoch keine Bewertungen
- Kendriya Vidyalaya Dipatoli Formative Assessment - III, (2015-16) Time-Class-V (FIVE) M.M - Grade A+ Subject - Environmental StudiesDokument5 SeitenKendriya Vidyalaya Dipatoli Formative Assessment - III, (2015-16) Time-Class-V (FIVE) M.M - Grade A+ Subject - Environmental StudiesSUBHANoch keine Bewertungen
- VSA - 1 Mark Questions Fill in The Blanks:: Kendriya Vidyalaya Sangathan, Chennai RegionDokument12 SeitenVSA - 1 Mark Questions Fill in The Blanks:: Kendriya Vidyalaya Sangathan, Chennai RegionSUBHANoch keine Bewertungen
- Boxes & SketchesDokument2 SeitenBoxes & SketchesSUBHANoch keine Bewertungen
- Kendriya Vidyalaya (Avadi Cluster)Dokument8 SeitenKendriya Vidyalaya (Avadi Cluster)SUBHANoch keine Bewertungen
- CBSE Class 1 Maths Chapter 10 WorksheetDokument10 SeitenCBSE Class 1 Maths Chapter 10 WorksheetSUBHANoch keine Bewertungen
- Class - V Mathematics Full Marks:190 Time: 3 HrsDokument13 SeitenClass - V Mathematics Full Marks:190 Time: 3 HrsSUBHANoch keine Bewertungen
- Practical Exam: Mark SchemeDokument14 SeitenPractical Exam: Mark SchemeSUBHANoch keine Bewertungen
- Topic: Counting in Groups: Counting by Two's Write Numbers Starting FromDokument2 SeitenTopic: Counting in Groups: Counting by Two's Write Numbers Starting FromSUBHANoch keine Bewertungen
- केंद्रीय विद्यालय / Class: V (FIVE) Time: 1 ½ Hours Subject: Mathematics Grade:A+ Name - - - - - - - - - - - - - - - - - - - - - - - Roll - - - - - - - -Dokument7 Seitenकेंद्रीय विद्यालय / Class: V (FIVE) Time: 1 ½ Hours Subject: Mathematics Grade:A+ Name - - - - - - - - - - - - - - - - - - - - - - - Roll - - - - - - - -SUBHANoch keine Bewertungen
- 5 EnglishDokument11 Seiten5 EnglishSUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Compound Interest Part 5Dokument3 SeitenAptitude Logical Reasoning Compound Interest Part 5SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Averages 2020 Competitive Exams Part 3Dokument4 SeitenAptitude Logical Reasoning Averages 2020 Competitive Exams Part 3SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Profit and Loss 2020 Competitive ExamsDokument4 SeitenAptitude Logical Reasoning Profit and Loss 2020 Competitive ExamsSUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Compound Interest Part 7Dokument5 SeitenAptitude Logical Reasoning Compound Interest Part 7SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Compound Interest Part 3Dokument5 SeitenAptitude Logical Reasoning Compound Interest Part 3SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Mixtures and Allegations 2020 Competitive Exams Part 2Dokument4 SeitenAptitude Logical Reasoning Mixtures and Allegations 2020 Competitive Exams Part 2SUBHANoch keine Bewertungen
- AIIMS Logical Reasoning Pipes and Cistern 2020 Part 2 Competitive ExamsDokument5 SeitenAIIMS Logical Reasoning Pipes and Cistern 2020 Part 2 Competitive ExamsSUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Compound Interest Part 6Dokument4 SeitenAptitude Logical Reasoning Compound Interest Part 6SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Pipes and Cisterns Part 3Dokument5 SeitenAptitude Logical Reasoning Pipes and Cisterns Part 3SUBHANoch keine Bewertungen
- AIIMS Logical Reasoning Pipes and Cistern 2020 Part 4 Competitive ExamsDokument2 SeitenAIIMS Logical Reasoning Pipes and Cistern 2020 Part 4 Competitive ExamsSUBHANoch keine Bewertungen
- AIIMS Logical Reasoning Pipes and Cistern 2020 Part 1 Competitive ExamsDokument5 SeitenAIIMS Logical Reasoning Pipes and Cistern 2020 Part 1 Competitive ExamsSUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Averages 2020 Competitive Exams Part 7Dokument3 SeitenAptitude Logical Reasoning Averages 2020 Competitive Exams Part 7SUBHANoch keine Bewertungen
- After A Bath: Text Based QuestionsDokument6 SeitenAfter A Bath: Text Based QuestionsSUBHA100% (2)
- Aptitude Logical Reasoning Averages 2020 Competitive Exams Part 2Dokument5 SeitenAptitude Logical Reasoning Averages 2020 Competitive Exams Part 2SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Averages 2020 Competitive Exams Part 1Dokument4 SeitenAptitude Logical Reasoning Averages 2020 Competitive Exams Part 1SUBHANoch keine Bewertungen
- Aptitude Logical Reasoning Averages Part 4Dokument5 SeitenAptitude Logical Reasoning Averages Part 4SUBHANoch keine Bewertungen
- Three Little Pigs: Text Based QuestionsDokument5 SeitenThree Little Pigs: Text Based QuestionsSUBHANoch keine Bewertungen
- One Little Kitten: Text Based QuestionsDokument5 SeitenOne Little Kitten: Text Based QuestionsSUBHANoch keine Bewertungen
- Master User Guide: Premier 412/816/832Dokument24 SeitenMaster User Guide: Premier 412/816/832وسام نصر يوسفNoch keine Bewertungen
- 1 General Information: Model Number Short Description Counter Functions Required Accessories Bus ModulesDokument11 Seiten1 General Information: Model Number Short Description Counter Functions Required Accessories Bus Modulesroni kurniawanNoch keine Bewertungen
- Lenovo Diagnostics - LOG: 3/16/2021 11:42:57 AM - PassedDokument12 SeitenLenovo Diagnostics - LOG: 3/16/2021 11:42:57 AM - PassedJosé Tomás FerrandoNoch keine Bewertungen
- TRAXPro ManualDokument86 SeitenTRAXPro ManualErlinangNoch keine Bewertungen
- MessageDokument87 SeitenMessageamdevaNoch keine Bewertungen
- Ch-3 & 4 Solving System of EquationsDokument18 SeitenCh-3 & 4 Solving System of EquationsAbel TayeNoch keine Bewertungen
- Fuzzy Self Tuning of PID ControllersDokument10 SeitenFuzzy Self Tuning of PID ControllersSeveriano Jaramillo QuintanarNoch keine Bewertungen
- Week 03 Assignment 03 PDFDokument4 SeitenWeek 03 Assignment 03 PDFRahul YadavNoch keine Bewertungen
- Ulss Ulsm UlslDokument1 SeiteUlss Ulsm UlslHamzaNoch keine Bewertungen
- Resume of Resource Person: Professional Regulation CommissionDokument3 SeitenResume of Resource Person: Professional Regulation CommissionMa. Jennyrose Solis100% (1)
- Computing For Scientists and Engineers A Workbook of Analysis, Numerics, and Applications (Thompson) (1992)Dokument458 SeitenComputing For Scientists and Engineers A Workbook of Analysis, Numerics, and Applications (Thompson) (1992)jumacoga100% (1)
- Lecture 8 - Goms IIDokument21 SeitenLecture 8 - Goms IIkipkoecharonz korirNoch keine Bewertungen
- FLAC2 DDokument180 SeitenFLAC2 DMohamed A. El-BadawiNoch keine Bewertungen
- Building A Ha and DR Solution Using Alwayson SQL Fcis and Ags v1Dokument37 SeitenBuilding A Ha and DR Solution Using Alwayson SQL Fcis and Ags v1Prasad ReddNoch keine Bewertungen
- Completing The SquareDokument17 SeitenCompleting The Squarezoha shahzadNoch keine Bewertungen
- Training Contents - WebmethodsDokument6 SeitenTraining Contents - WebmethodsShyamini Dhinesh0% (1)
- Seatupjee Poly Jan1316Dokument63 SeitenSeatupjee Poly Jan1316Arshdeep YadavNoch keine Bewertungen
- An Assignment Problem Is A Particular Case of Transportation ProblemDokument7 SeitenAn Assignment Problem Is A Particular Case of Transportation ProblemsunilsinghmNoch keine Bewertungen
- Concept of ERS in SAP MMDokument9 SeitenConcept of ERS in SAP MMARABINDA CHAKRAVARTYNoch keine Bewertungen
- Mecapion Servo Motors 2012Dokument68 SeitenMecapion Servo Motors 2012GianLucaNoch keine Bewertungen
- Tomorrow'S Technology For Today'S Security: Product HighlightsDokument2 SeitenTomorrow'S Technology For Today'S Security: Product HighlightsBanu AtamNoch keine Bewertungen
- The Importance of Basic Printing Education For Human Resource Development in Printing IndustryDokument12 SeitenThe Importance of Basic Printing Education For Human Resource Development in Printing IndustryAries Chandra AnandithaNoch keine Bewertungen
- Enlaces Descargas Windows Dan RatiaDokument4 SeitenEnlaces Descargas Windows Dan RatiaEnrique LinerosNoch keine Bewertungen
- Manual Cantar Electronic Dibal VD-310Dokument34 SeitenManual Cantar Electronic Dibal VD-310Prima VD50% (2)
- Accenture Methodology Training Part 01Dokument12 SeitenAccenture Methodology Training Part 01Christophe MarinoNoch keine Bewertungen
- Interview Transcript - David DanksDokument11 SeitenInterview Transcript - David DanksJoon JangNoch keine Bewertungen
- Usermanual SHD-8900 Alien en v120921Dokument37 SeitenUsermanual SHD-8900 Alien en v120921yul2kNoch keine Bewertungen
- Soc BookDokument19 SeitenSoc BookmuraliNoch keine Bewertungen
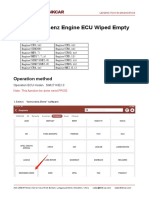
- Mercedes Benz Engine ECU Wiped EmptyDokument9 SeitenMercedes Benz Engine ECU Wiped EmptyP BNoch keine Bewertungen
- Huawei OMC IManager M2000 Engineering Parameters IntroductionDokument11 SeitenHuawei OMC IManager M2000 Engineering Parameters IntroductionaricomenNoch keine Bewertungen