Das könnte Ihnen auch gefallen
- Class II, Division 1, Case With Multiple Treatment ChallengesDokument5 SeitenClass II, Division 1, Case With Multiple Treatment ChallengesBagis Emre GulNoch keine Bewertungen
- 1999 115 3 227 232 FernandesDokument6 Seiten1999 115 3 227 232 FernandesBagis Emre GulNoch keine Bewertungen
- 1999 115 2 125 132 MeehanDokument8 Seiten1999 115 2 125 132 MeehanBagis Emre GulNoch keine Bewertungen
- Mand Incisor ExtDokument12 SeitenMand Incisor ExtLanaNoch keine Bewertungen
- 1999 115 2 138 142 NakamuraDokument5 Seiten1999 115 2 138 142 NakamuraBagis Emre GulNoch keine Bewertungen
- Orthodontics: A Case Study in The Tension Between Guild Standards and CapitalismDokument2 SeitenOrthodontics: A Case Study in The Tension Between Guild Standards and CapitalismBagis Emre GulNoch keine Bewertungen
- 1999 115 1 83 88 MiyawakiDokument6 Seiten1999 115 1 83 88 MiyawakiBagis Emre GulNoch keine Bewertungen
- Craniofacial Adaptations Induced by Chincup Therapy in Class III PatientsDokument8 SeitenCraniofacial Adaptations Induced by Chincup Therapy in Class III PatientsAlla MushkeyNoch keine Bewertungen
- Impact Resistance of Ceramic Brackets According To Ophthalmic Lenses StandardsDokument8 SeitenImpact Resistance of Ceramic Brackets According To Ophthalmic Lenses StandardsBagis Emre GulNoch keine Bewertungen
- 1999 115 1 72 76 Jr.,-McNamaraDokument5 Seiten1999 115 1 72 76 Jr.,-McNamaraBagis Emre GulNoch keine Bewertungen
- 1999 115 1 55 60 HansenDokument6 Seiten1999 115 1 55 60 HansenBagis Emre GulNoch keine Bewertungen
- The International Journal of Periodontics & Restorative DentistryDokument9 SeitenThe International Journal of Periodontics & Restorative DentistryBagis Emre GulNoch keine Bewertungen
- 1999 115 2 166 174 UmemoriDokument9 Seiten1999 115 2 166 174 UmemoriBagis Emre GulNoch keine Bewertungen
- A Longitudinal Cephalometric Study of Postorthodontic Craniofacial ChangesDokument6 SeitenA Longitudinal Cephalometric Study of Postorthodontic Craniofacial ChangesBagis Emre GulNoch keine Bewertungen
- 10 11607@prd 3968Dokument8 Seiten10 11607@prd 3968Bagis Emre GulNoch keine Bewertungen
- American Journal of Orthodontics and Dentofacial OrthopedicsDokument3 SeitenAmerican Journal of Orthodontics and Dentofacial OrthopedicsBagis Emre GulNoch keine Bewertungen
- 1999 115 1 89 98 MarotoDokument10 Seiten1999 115 1 89 98 MarotoAlla MushkeyNoch keine Bewertungen
- 1999 115 1 13 23 NelsonDokument11 Seiten1999 115 1 13 23 NelsonAlla MushkeyNoch keine Bewertungen
- Shear Bond Strength of Composite, Glass Ionomer, and Acidic Primer Adhesive SystemsDokument5 SeitenShear Bond Strength of Composite, Glass Ionomer, and Acidic Primer Adhesive SystemsRaluca GrigoreNoch keine Bewertungen
- 1999 115 1 29 38 ChangDokument10 Seiten1999 115 1 29 38 ChangAlla MushkeyNoch keine Bewertungen
- The International Journal of Periodontics & Restorative DentistryDokument8 SeitenThe International Journal of Periodontics & Restorative DentistryBagis Emre GulNoch keine Bewertungen
- Implantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesDokument8 SeitenImplantoplasty Enhancing Peri-Implant Bone Stability Over A 3-Year Follow-Up: A Case SeriesBagis Emre GulNoch keine Bewertungen
- Article PDFDokument12 SeitenArticle PDFJames LinNoch keine Bewertungen
- 1999 115 1 39 51 ArticoloDokument13 Seiten1999 115 1 39 51 ArticoloBagis Emre GulNoch keine Bewertungen
- 1999 115 1 1 12 Figueroa PDFDokument12 Seiten1999 115 1 1 12 Figueroa PDFAlla MushkeyNoch keine Bewertungen
- Physical-Chemical Analyses of Contaminations and Internal Holes in Dental Implants of Pure Commercial TitaniumDokument7 SeitenPhysical-Chemical Analyses of Contaminations and Internal Holes in Dental Implants of Pure Commercial TitaniumBagis Emre GulNoch keine Bewertungen
- Editorial: Developing A Consensus: Abutment/Crown Design For Single-Tooth Implant RestorationsDokument1 SeiteEditorial: Developing A Consensus: Abutment/Crown Design For Single-Tooth Implant RestorationsBagis Emre GulNoch keine Bewertungen
- In Vitro Analysis of The Fracture Resistance of CAD-CAM Monolithic Lithium Disilicate Molar Crowns With Different Occlusal ThicknessDokument7 SeitenIn Vitro Analysis of The Fracture Resistance of CAD-CAM Monolithic Lithium Disilicate Molar Crowns With Different Occlusal ThicknessBagis Emre GulNoch keine Bewertungen
- Photoelastic Analysis of Dynamic Stress Distribution Around Short Implants Restored With Different MaterialsDokument6 SeitenPhotoelastic Analysis of Dynamic Stress Distribution Around Short Implants Restored With Different MaterialsBagis Emre GulNoch keine Bewertungen
- Inter-Occlusal Appliance For Implant Site Augmentation and Optimal Implant Positioning A Ten-Year Follow-Up Case ReportDokument7 SeitenInter-Occlusal Appliance For Implant Site Augmentation and Optimal Implant Positioning A Ten-Year Follow-Up Case ReportBagis Emre GulNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Eating Disorders Eating Disorders OverviewDokument12 SeitenEating Disorders Eating Disorders OverviewGiancarlo CrespoNoch keine Bewertungen
- VTR 214 PDFDokument2 SeitenVTR 214 PDFKimberly AndrzejewskiNoch keine Bewertungen
- Pcap - PathophysiologyDokument4 SeitenPcap - PathophysiologyAyla Mar100% (1)
- Case Study Formate MSNDokument2 SeitenCase Study Formate MSNLijoNoch keine Bewertungen
- Sitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsDokument28 SeitenSitecore - Media Library - Files.3d Imaging - Shared.7701 3dbrochure UsandiNoch keine Bewertungen
- Impared NursesDokument11 SeitenImpared Nursesapi-240352043Noch keine Bewertungen
- Delivery Room Emergencies: Amanda Louise Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistDokument44 SeitenDelivery Room Emergencies: Amanda Louise Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistLyn LynNoch keine Bewertungen
- ThoracentesisDokument1 SeiteThoracentesisNiño Cris PatiñoNoch keine Bewertungen
- PartografDokument31 SeitenPartografrovi wilmanNoch keine Bewertungen
- APA - DSM5 - Level 2 Inattention Parent of Child Age 6 To 17 PDFDokument3 SeitenAPA - DSM5 - Level 2 Inattention Parent of Child Age 6 To 17 PDFLiana Storm0% (1)
- Learning Area Grade Level Quarter Date I. Lesson Title Ii. Most Essential Learning Competencies (Melcs)Dokument4 SeitenLearning Area Grade Level Quarter Date I. Lesson Title Ii. Most Essential Learning Competencies (Melcs)Ashly RoderosNoch keine Bewertungen
- Nursing Theorists (W/ Their Theory/model) : Faye Glenn Abdellah Dorothy Johnson Imogene KingDokument3 SeitenNursing Theorists (W/ Their Theory/model) : Faye Glenn Abdellah Dorothy Johnson Imogene KingRodel P. Elep IIINoch keine Bewertungen
- Lesson Plan On Minor Disorders During Pregnancy Its Management 1Dokument20 SeitenLesson Plan On Minor Disorders During Pregnancy Its Management 1Bhawna Joshi100% (6)
- Diabetic Ketoacidosis - WikipediaDokument32 SeitenDiabetic Ketoacidosis - WikipediaSanket TelangNoch keine Bewertungen
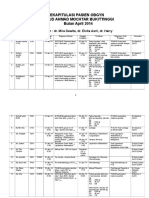
- Rekapitulasi Pasien Obgyn Apr 2014 2Dokument20 SeitenRekapitulasi Pasien Obgyn Apr 2014 2Ressy Dara AmeliaNoch keine Bewertungen
- 1-Diabetes Package - PO2693771771-269Dokument6 Seiten1-Diabetes Package - PO2693771771-269KishoreNoch keine Bewertungen
- Dip HIV Man (SA) Regulations 24-1-2017Dokument9 SeitenDip HIV Man (SA) Regulations 24-1-2017matentenNoch keine Bewertungen
- Modul Bahasa Inggris Kep-D3 Sem 4Dokument32 SeitenModul Bahasa Inggris Kep-D3 Sem 4Mufarroha98Noch keine Bewertungen
- Breast Feeding ModifiedDokument16 SeitenBreast Feeding ModifiedTilahun Mikias100% (1)
- Dermatological Signs in Wilson's DiseaseDokument4 SeitenDermatological Signs in Wilson's DiseaseGingerWiseNoch keine Bewertungen
- Diagnosis and Management of Fetal Mummification in CowDokument5 SeitenDiagnosis and Management of Fetal Mummification in CowAbdul Wahab Assya RoniNoch keine Bewertungen
- HYPOTHYROIDISMDokument11 SeitenHYPOTHYROIDISMVarun SinghNoch keine Bewertungen
- Guidance COVID-19Dokument5 SeitenGuidance COVID-19hemkumar DahalNoch keine Bewertungen
- Vasopressors For ShockDokument21 SeitenVasopressors For ShocknugrahaNoch keine Bewertungen
- Int Endodontic J - 2022 - Shah - Outcomes Reporting in Systematic Reviews On Surgical Endodontics A Scoping Review For TheDokument22 SeitenInt Endodontic J - 2022 - Shah - Outcomes Reporting in Systematic Reviews On Surgical Endodontics A Scoping Review For TheDhiaa AloweadatNoch keine Bewertungen
- LeukocoriaDokument5 SeitenLeukocoriabahaashakirNoch keine Bewertungen
- News Story 3Dokument2 SeitenNews Story 3api-558280939Noch keine Bewertungen
- Patient Record BookDokument1 SeitePatient Record BooksumarumNoch keine Bewertungen
- Four Big Pollution Diseases of Japan - Wikipedia, The Free Encyclopedia PDFDokument6 SeitenFour Big Pollution Diseases of Japan - Wikipedia, The Free Encyclopedia PDFudayngNoch keine Bewertungen
- The Three Basic Components of A Pulse: Shape, Jump, and LevelDokument3 SeitenThe Three Basic Components of A Pulse: Shape, Jump, and LevelShahul Hameed100% (1)