Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDokument8 SeitenFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752Noch keine Bewertungen
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDokument5 SeitenTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752Noch keine Bewertungen
- (2012) Investigation and Management of Splenic Disease in DogsDokument8 Seiten(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography - The SpleenDokument9 SeitenSmall Animal Abdominal Ultrasonography - The Spleenludiegues752Noch keine Bewertungen
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDokument3 Seiten(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Noch keine Bewertungen
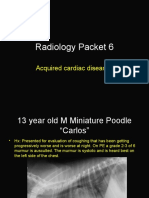
- Radiology Packet 6 Acquired Cardiac DiseasesDokument25 SeitenRadiology Packet 6 Acquired Cardiac Diseasesludiegues752Noch keine Bewertungen
- Radiology Packet 7 Congenital Cardiac DiseaseDokument27 SeitenRadiology Packet 7 Congenital Cardiac Diseaseludiegues752Noch keine Bewertungen
- US Artifacts - University of ChicagoDokument101 SeitenUS Artifacts - University of Chicagoludiegues752Noch keine Bewertungen
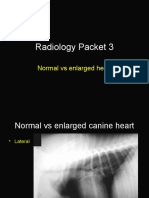
- Radiology Packet 3 Normal Vs Enlarged HeartDokument11 SeitenRadiology Packet 3 Normal Vs Enlarged Heartludiegues752Noch keine Bewertungen
- Imaging Intestinal ObstructionDokument5 SeitenImaging Intestinal Obstructionludiegues752Noch keine Bewertungen
- Radiology Packet 5: Heart Failure CasesDokument25 SeitenRadiology Packet 5: Heart Failure Casesludiegues752Noch keine Bewertungen
- Radiology Packet 4 Cardiac CasesDokument28 SeitenRadiology Packet 4 Cardiac Casesludiegues752Noch keine Bewertungen
- (2012) Investigation and Management of Splenic Disease in DogsDokument8 Seiten(2012) Investigation and Management of Splenic Disease in Dogsludiegues752Noch keine Bewertungen
- Ultrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal DogsDokument10 SeitenUltrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal Dogsludiegues752Noch keine Bewertungen
- (2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland IllnessDokument9 Seiten(2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland Illnessludiegues752Noch keine Bewertungen
- (2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting AdenomaDokument5 Seiten(2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting Adenomaludiegues752Noch keine Bewertungen
- Dermatology History FormDokument1 SeiteDermatology History Formludiegues752Noch keine Bewertungen
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDokument3 Seiten(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752Noch keine Bewertungen
- Dog with Lung Mineralization from Steroid TherapyDokument4 SeitenDog with Lung Mineralization from Steroid Therapyludiegues752Noch keine Bewertungen
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDokument5 Seiten(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752Noch keine Bewertungen
- (2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFDokument6 Seiten(2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFludiegues752Noch keine Bewertungen
- (2015) Basics of Equine DermatologyDokument10 Seiten(2015) Basics of Equine Dermatologyludiegues752Noch keine Bewertungen
- (2012) Emerging Skin Conditions in CattleDokument9 Seiten(2012) Emerging Skin Conditions in Cattleludiegues752Noch keine Bewertungen
- (2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking DiseasesDokument5 Seiten(2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking Diseasesludiegues752Noch keine Bewertungen
- (1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal DiseaseDokument7 Seiten(1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal Diseaseludiegues752Noch keine Bewertungen
- Alterations in The SkinDokument9 SeitenAlterations in The Skinludiegues752Noch keine Bewertungen
- The IntegumentDokument15 SeitenThe Integumentludiegues752Noch keine Bewertungen
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDokument5 SeitenSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752Noch keine Bewertungen
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Dokument8 SeitenSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Grading ScaleDokument2 SeitenGrading ScaleFelipe SanchezNoch keine Bewertungen
- Case StudyDokument4 SeitenCase StudyCOLLEENKATE ARMENDINoch keine Bewertungen
- Squamous Papilloma On Hard Palate: Case Report and Literature ReviewDokument3 SeitenSquamous Papilloma On Hard Palate: Case Report and Literature ReviewadelNoch keine Bewertungen
- Review of Mirizzi Syndrome Classification and PresentationDokument5 SeitenReview of Mirizzi Syndrome Classification and PresentationNovi WiarniNoch keine Bewertungen
- InmjDokument8 SeitenInmjParth100% (2)
- Chapter 4 Social Pharmacy Introduction To Microbiology and Common NoteskartsDokument6 SeitenChapter 4 Social Pharmacy Introduction To Microbiology and Common NoteskartsSushovan AshNoch keine Bewertungen
- Radicular SyndromeDokument40 SeitenRadicular Syndromeainulhawa89Noch keine Bewertungen
- Warwick Boulevard, Newport News, VA 23606-3401 Phone: 757-591-4646Dokument2 SeitenWarwick Boulevard, Newport News, VA 23606-3401 Phone: 757-591-4646Rosaline JordanNoch keine Bewertungen
- Buy Renew Service Claim queries for ICICI Lombard Health InsuranceDokument4 SeitenBuy Renew Service Claim queries for ICICI Lombard Health InsuranceMonal RajNoch keine Bewertungen
- Transposition of The Great Arteries (TGA)Dokument4 SeitenTransposition of The Great Arteries (TGA)Tommy JohnsonNoch keine Bewertungen
- Pathology Course Audit-3Dokument26 SeitenPathology Course Audit-3Joana Marie PalatanNoch keine Bewertungen
- Health 8 Q3 TGDokument67 SeitenHealth 8 Q3 TGAngelica TumamakNoch keine Bewertungen
- Complete Revision Notes by Vincent Helyar and Aidan Shaw 2018Dokument645 SeitenComplete Revision Notes by Vincent Helyar and Aidan Shaw 2018Zubair Lone100% (4)
- HEALTH QUESTIONNAIRE (Talatanungan Ukol Sa Kalusugan) :: Please Read Carefully (Basahin NG Mabuti)Dokument2 SeitenHEALTH QUESTIONNAIRE (Talatanungan Ukol Sa Kalusugan) :: Please Read Carefully (Basahin NG Mabuti)Karen Kaye PasamonteNoch keine Bewertungen
- 3 - 500 MCQs PDFDokument140 Seiten3 - 500 MCQs PDFmusman1947100% (1)
- MSNHaemorrhoidsDokument17 SeitenMSNHaemorrhoidsBrittany JordanNoch keine Bewertungen
- 2017 AAS ProgramDokument20 Seiten2017 AAS ProgramSiddharth NandaNoch keine Bewertungen
- SarcoidosisDokument17 SeitenSarcoidosisapi-678326591Noch keine Bewertungen
- NCP AgnDokument2 SeitenNCP Agnj3nann3Noch keine Bewertungen
- Hallucinations: Soundarya. A - N Roll No.: 112Dokument17 SeitenHallucinations: Soundarya. A - N Roll No.: 112Jayashree goveraNoch keine Bewertungen
- Ovarian Cancer Antigen (Ca-125) : Enzyme Immunoassay Test Kit Catalog Number: 10103Dokument2 SeitenOvarian Cancer Antigen (Ca-125) : Enzyme Immunoassay Test Kit Catalog Number: 10103yousrazeidan1979Noch keine Bewertungen
- Dysphagia Case StudyDokument12 SeitenDysphagia Case Studyapi-340845010Noch keine Bewertungen
- ValdecoxibDokument3 SeitenValdecoxibapi-3797941Noch keine Bewertungen
- DARUNDAY SICwatDokument12 SeitenDARUNDAY SICwatEzra Miguel DarundayNoch keine Bewertungen
- Nursing Care Plan: Student's Name: ID: Course Name: SettingDokument3 SeitenNursing Care Plan: Student's Name: ID: Course Name: SettingnjoodNoch keine Bewertungen
- NizoralDokument4 SeitenNizoralianecunar100% (2)
- HERNIA - Case StudyDokument8 SeitenHERNIA - Case StudyMa Jaimeliz Mae MuñizNoch keine Bewertungen
- Severe Sepsis Screening Tool NhsDokument2 SeitenSevere Sepsis Screening Tool NhsDavide Antonelli LaghiNoch keine Bewertungen
- Dysphagia AssessmentDokument6 SeitenDysphagia AssessmentShruti PatilNoch keine Bewertungen
- Infection Control in Dental RadiologyDokument41 SeitenInfection Control in Dental RadiologyDrShweta Saini0% (1)