Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Patients Are Not The EnemyDokument3 SeitenPatients Are Not The EnemyLaurian VegaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Ozone Widget Framework: Towards Modularity of C2 Human InterfacesDokument6 SeitenThe Ozone Widget Framework: Towards Modularity of C2 Human InterfacesLaurian VegaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Time ManagementDokument3 SeitenTime ManagementLaurian VegaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Confidence PanelDokument3 SeitenConfidence PanelLaurian VegaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Patient Trust and Health WebsitesDokument15 SeitenPatient Trust and Health WebsitesLaurian VegaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Final-Trial by DiaperDokument3 SeitenFinal-Trial by DiaperLaurian VegaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Security in Practice: Examining The Collaborative Management of Personal Sensitive Information in Childcare Centers and Physician's Offices, PresentationDokument102 SeitenSecurity in Practice: Examining The Collaborative Management of Personal Sensitive Information in Childcare Centers and Physician's Offices, PresentationLaurian VegaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- CHIMe PosterDokument1 SeiteCHIMe PosterLaurian VegaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Baby ReloadingDokument3 SeitenBaby ReloadingLaurian VegaNoch keine Bewertungen
- Security in Practice: Examining The Collaborative Management of Sensitive Information in Childcare Centers and Physicians' OfficesDokument386 SeitenSecurity in Practice: Examining The Collaborative Management of Sensitive Information in Childcare Centers and Physicians' OfficesLaurian VegaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Security Practice: Design, Adoption, and Use of Technology For Collaboratively Managing Sensitive Personal Information - PresentationDokument14 SeitenSecurity Practice: Design, Adoption, and Use of Technology For Collaboratively Managing Sensitive Personal Information - PresentationLaurian VegaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
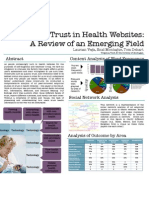
- Trust in Health Websites: A Review of An Emerging FieldDokument1 SeiteTrust in Health Websites: A Review of An Emerging FieldLaurian VegaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Laurian Vega Research Defense PresentationDokument58 SeitenLaurian Vega Research Defense PresentationLaurian VegaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Babies in Graduate School: Making It HappenDokument15 SeitenBabies in Graduate School: Making It HappenLaurian VegaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Mommies Know Best: Continuing The Discussion On Pregnancy and Graduate School, PresentationDokument20 SeitenMommies Know Best: Continuing The Discussion On Pregnancy and Graduate School, PresentationLaurian VegaNoch keine Bewertungen
- Security Practice: Design, Adoption, and Use of Technology For Collaboratively Managing Sensitive Personal InformationDokument5 SeitenSecurity Practice: Design, Adoption, and Use of Technology For Collaboratively Managing Sensitive Personal InformationLaurian VegaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Usable Security in Practice: Collaborative Management of Electronic & Physical Personal Information - PresentationDokument20 SeitenUsable Security in Practice: Collaborative Management of Electronic & Physical Personal Information - PresentationLaurian VegaNoch keine Bewertungen
- "I Don't Necessarily Trust My Childcare": Securing Electronic & Physical Sensitive InformationDokument3 Seiten"I Don't Necessarily Trust My Childcare": Securing Electronic & Physical Sensitive InformationLaurian VegaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Trust in Health Websites: A Review of An Emerging FieldDokument10 SeitenTrust in Health Websites: A Review of An Emerging FieldLaurian VegaNoch keine Bewertungen
- Wiimote PresentationDokument1 SeiteWiimote PresentationLaurian VegaNoch keine Bewertungen
- Baby Reloading 1 Page AbstractDokument1 SeiteBaby Reloading 1 Page AbstractLaurian VegaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Zones of Ambiguity DealersDokument24 SeitenZones of Ambiguity DealersLaurian VegaNoch keine Bewertungen
- Usable Security in Practice: Collaborative Management of Electronic & Physical Personal Information.Dokument3 SeitenUsable Security in Practice: Collaborative Management of Electronic & Physical Personal Information.Laurian VegaNoch keine Bewertungen
- Security in Practice: Examining The Collaborative Management of Personal Sensitive Information in Childcares and Medical Centers, Dissertation ProposalDokument104 SeitenSecurity in Practice: Examining The Collaborative Management of Personal Sensitive Information in Childcares and Medical Centers, Dissertation ProposalLaurian VegaNoch keine Bewertungen
- TIME: A Method of Detecting The Dynamic Variances of TrustDokument8 SeitenTIME: A Method of Detecting The Dynamic Variances of TrustLaurian VegaNoch keine Bewertungen
- T.I.M.E: A Method of Detecting The Dynamic Variances of TrustDokument57 SeitenT.I.M.E: A Method of Detecting The Dynamic Variances of TrustLaurian VegaNoch keine Bewertungen
- CHIMe PosterDokument1 SeiteCHIMe PosterLaurian VegaNoch keine Bewertungen
- LCV Dissertation Proposal PresentationDokument53 SeitenLCV Dissertation Proposal PresentationLaurian VegaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Securing Sensitive Information in Work PracticeDokument10 SeitenSecuring Sensitive Information in Work PracticeLaurian VegaNoch keine Bewertungen
- Total English Placement TestDokument6 SeitenTotal English Placement TestKaterina PapakonstantinouNoch keine Bewertungen
- Alphabet Series Tricks - PDF: Down During Your ExamDokument8 SeitenAlphabet Series Tricks - PDF: Down During Your ExamJoshNoch keine Bewertungen
- Behind The Scrubs: Monica Velarde Saint Mary's College December 09, 2008Dokument21 SeitenBehind The Scrubs: Monica Velarde Saint Mary's College December 09, 2008EthanNoch keine Bewertungen
- Do Large Language Models Need Sensory Grounding For Meaning and Understanding?Dokument38 SeitenDo Large Language Models Need Sensory Grounding For Meaning and Understanding?Zakhar KoganNoch keine Bewertungen
- Civil Law - Persons FamilyDokument59 SeitenCivil Law - Persons FamilyCharmaine MejiaNoch keine Bewertungen
- Global University Rankings and Their ImpactDokument85 SeitenGlobal University Rankings and Their ImpactКино ФильмNoch keine Bewertungen
- Dallas Baptist University Writing Center: Narrative EssayDokument3 SeitenDallas Baptist University Writing Center: Narrative EssayumagandhiNoch keine Bewertungen
- People V DueroDokument5 SeitenPeople V DueroJazem AnsamaNoch keine Bewertungen
- The Importance of Instructional MaterialDokument3 SeitenThe Importance of Instructional MaterialJheramae SegoviaNoch keine Bewertungen
- Compressible Potential FlowDokument15 SeitenCompressible Potential FlowChanoNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jean Faber and Gilson A. Giraldi - Quantum Models For Artifcial Neural NetworkDokument8 SeitenJean Faber and Gilson A. Giraldi - Quantum Models For Artifcial Neural Networkdcsi3Noch keine Bewertungen
- Presumption - Person Possession A Falsified Document and Be Made Use of It, He Is The Material Author of The FalsificationDokument3 SeitenPresumption - Person Possession A Falsified Document and Be Made Use of It, He Is The Material Author of The FalsificationbeabineneNoch keine Bewertungen
- Malatras ChristosDokument13 SeitenMalatras Christosdimco2007Noch keine Bewertungen
- Powerful Hero Dpa Rtsal Protective DeityDokument50 SeitenPowerful Hero Dpa Rtsal Protective DeityjinpaNoch keine Bewertungen
- Classical Vs KeynisianDokument8 SeitenClassical Vs KeynisianRinky BhattacharyaNoch keine Bewertungen
- Scanner Hardware Stopped Scan - Replace Collimator CAM (A - B) Motor and Coupling AssemblyDokument5 SeitenScanner Hardware Stopped Scan - Replace Collimator CAM (A - B) Motor and Coupling AssemblyLuis BattaNoch keine Bewertungen
- CC 109 - MLGCLDokument25 SeitenCC 109 - MLGCLClark QuayNoch keine Bewertungen
- Training Needs in Facilities Management Zaharah Manaf 2005Dokument11 SeitenTraining Needs in Facilities Management Zaharah Manaf 2005Anonymous dmYc1M4uNoch keine Bewertungen
- Deluxe SolutionDokument6 SeitenDeluxe SolutionR K Patham100% (1)
- Zambian Open University: School of Social Science and HumanitiesDokument9 SeitenZambian Open University: School of Social Science and HumanitiesEvangelist Kabaso SydneyNoch keine Bewertungen
- IA Feedback Template RevisedDokument1 SeiteIA Feedback Template RevisedtyrramNoch keine Bewertungen
- Rectification of Errors - QuestionsDokument6 SeitenRectification of Errors - QuestionsBhargav RavalNoch keine Bewertungen
- Web Applications Desktop IntegratorDokument5 SeitenWeb Applications Desktop IntegratorSatendra BhatiNoch keine Bewertungen
- OODBSDokument29 SeitenOODBSMinh Tu TranNoch keine Bewertungen
- EDEL453 Spring2013 MelanieHADJES Unit 4 Economic Day1Dokument6 SeitenEDEL453 Spring2013 MelanieHADJES Unit 4 Economic Day1Melanie HadjesNoch keine Bewertungen
- Project ExtensionDokument27 SeitenProject Extensionrajith rajeevNoch keine Bewertungen
- Omer Farooq ResumeDokument3 SeitenOmer Farooq ResumemykdesignerNoch keine Bewertungen
- Fabrication and Characterization of Polysilane PCBM Bulk Heterojunction Solar CellsDokument5 SeitenFabrication and Characterization of Polysilane PCBM Bulk Heterojunction Solar CellsHERNANDEZ1010Noch keine Bewertungen
- Rodriguez v. TorenoDokument2 SeitenRodriguez v. TorenoJerry CaneNoch keine Bewertungen
- Nervous System Regulating Activities by UnyteDokument14 SeitenNervous System Regulating Activities by UnytehellozenbokNoch keine Bewertungen
- The Internet Con: How to Seize the Means of ComputationVon EverandThe Internet Con: How to Seize the Means of ComputationBewertung: 5 von 5 Sternen5/5 (6)
- Defensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityVon EverandDefensive Cyber Mastery: Expert Strategies for Unbeatable Personal and Business SecurityBewertung: 5 von 5 Sternen5/5 (1)
- Practical Industrial Cybersecurity: ICS, Industry 4.0, and IIoTVon EverandPractical Industrial Cybersecurity: ICS, Industry 4.0, and IIoTNoch keine Bewertungen
- Hacking : The Ultimate Comprehensive Step-By-Step Guide to the Basics of Ethical HackingVon EverandHacking : The Ultimate Comprehensive Step-By-Step Guide to the Basics of Ethical HackingBewertung: 5 von 5 Sternen5/5 (3)
- Coding Democracy: How a Growing Hacking Movement is Disrupting Concentrations of Power, Mass Surveillance, and Authoritarianism in the Digital AgeVon EverandCoding Democracy: How a Growing Hacking Movement is Disrupting Concentrations of Power, Mass Surveillance, and Authoritarianism in the Digital AgeBewertung: 4.5 von 5 Sternen4.5/5 (3)