Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- ACS Case StudyDokument26 SeitenACS Case StudyMari Lyn100% (1)
- Nursing Responsibilities After CCDokument5 SeitenNursing Responsibilities After CCSofia P. PanlilioNoch keine Bewertungen
- Acute Coronary SyndromeDokument8 SeitenAcute Coronary SyndromeMohammad Neyazur RahamanNoch keine Bewertungen
- Maslaris 2018Dokument15 SeitenMaslaris 2018Jairo GuevaraNoch keine Bewertungen
- Thesis On Acute Coronary SyndromeDokument5 SeitenThesis On Acute Coronary Syndromejum1p0tonip3100% (2)
- Andrei Schwartz The Cardiogenic Shock What Is New in The TreatmentDokument32 SeitenAndrei Schwartz The Cardiogenic Shock What Is New in The TreatmentAdrian AfloroaeiNoch keine Bewertungen
- Care of The Post-Thrombectomy Patient: Topical ReviewDokument7 SeitenCare of The Post-Thrombectomy Patient: Topical ReviewBasilio BabarNoch keine Bewertungen
- Ischemic Heart DiseaseDokument56 SeitenIschemic Heart DiseaseSMART PHARMACY By BRIJESHNoch keine Bewertungen
- STEMI GuidelinesDokument32 SeitenSTEMI GuidelinesNurul FadhilahNoch keine Bewertungen
- ACSDokument56 SeitenACSGabriel CalderónNoch keine Bewertungen
- Ischaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeDokument104 SeitenIschaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeputriluftiNoch keine Bewertungen
- The OMI Manifesto PDF 3.29.18Dokument39 SeitenThe OMI Manifesto PDF 3.29.18LeonardoCampanelliNoch keine Bewertungen
- Mechanical Thrombectomy For Acute Ischemic StrokeDokument19 SeitenMechanical Thrombectomy For Acute Ischemic StrokeCarlos Alfredo Vargas QuinteroNoch keine Bewertungen
- Neuroimaging of Acute Ischemic Stroke Multimodal Imaging Approach For Acute Endovascular TherapyDokument17 SeitenNeuroimaging of Acute Ischemic Stroke Multimodal Imaging Approach For Acute Endovascular TherapyEliana NataliaNoch keine Bewertungen
- TOE Liver TransplantDokument10 SeitenTOE Liver TransplantpcarrascoeNoch keine Bewertungen
- Mechanical Thrombectomy For Acute Ischemic Stroke - UpToDateDokument20 SeitenMechanical Thrombectomy For Acute Ischemic Stroke - UpToDateisabel pangNoch keine Bewertungen
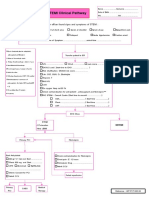
- STEMI Clinical PathwayDokument1 SeiteSTEMI Clinical PathwayKanoknun PisitpatcaragulNoch keine Bewertungen
- Facilitated Pci Vs Rescue Pci - DR Dolly MathewDokument51 SeitenFacilitated Pci Vs Rescue Pci - DR Dolly MathewJose JacobNoch keine Bewertungen
- Anderson 2017Dokument24 SeitenAnderson 2017muh.fitrah ramadanNoch keine Bewertungen
- Management of Acute MI, Role of Streptokinase, NicvdDokument22 SeitenManagement of Acute MI, Role of Streptokinase, NicvdNavojit ChowdhuryNoch keine Bewertungen
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDokument20 SeitenSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaNoch keine Bewertungen
- Overview of Mechanical Thrombectomy TechniquesDokument8 SeitenOverview of Mechanical Thrombectomy Techniquesjaknews adminNoch keine Bewertungen
- Overview of The Acute Management of ST-elevation Myocardial Infarction - UpToDateDokument25 SeitenOverview of The Acute Management of ST-elevation Myocardial Infarction - UpToDateMarcela Garzon O VelezNoch keine Bewertungen
- Acute Coronary SyndromeDokument9 SeitenAcute Coronary SyndromeAnthony Philip Patawaran CalimagNoch keine Bewertungen
- Acute Miocard InfarkDokument32 SeitenAcute Miocard InfarkhansNoch keine Bewertungen
- The Role of Magnesium in Clinical PracticeDokument20 SeitenThe Role of Magnesium in Clinical PracticeMagdalena Dwiyani HutajuluNoch keine Bewertungen
- Jakarta Cardiovascular Care Unit Network System PDFDokument52 SeitenJakarta Cardiovascular Care Unit Network System PDFekaNoch keine Bewertungen
- Acute Coronary Syndrome: Indra PrasetyaDokument92 SeitenAcute Coronary Syndrome: Indra PrasetyaPD-A UB 2017Noch keine Bewertungen
- Acute Ischaemic Stroke: Challenges For The IntensivistDokument13 SeitenAcute Ischaemic Stroke: Challenges For The IntensivistDobson Flores AparicioNoch keine Bewertungen
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDokument51 SeitenCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiNoch keine Bewertungen