Das könnte Ihnen auch gefallen
- UWorld NCLEX-RN QBank 2018 PDFDokument103 SeitenUWorld NCLEX-RN QBank 2018 PDFIlluminatis99% (90)
- StudyGuide BurnsDokument2 SeitenStudyGuide BurnsJm CoguincoNoch keine Bewertungen
- Orthopedic Nursing. Lecture Notes at Philipine Orthopedic CenterDokument7 SeitenOrthopedic Nursing. Lecture Notes at Philipine Orthopedic Centerhannjazz100% (5)
- NCLEX Cram SheetDokument8 SeitenNCLEX Cram SheetKaloy Kamao100% (5)
- All Character Builds GuideDokument102 SeitenAll Character Builds GuideJm CoguincoNoch keine Bewertungen
- Orthopedic NursingDokument9 SeitenOrthopedic Nursingsilimaanghang100% (2)
- Medical Surgical Nursing Orthopedic NursingDokument141 SeitenMedical Surgical Nursing Orthopedic Nursingroger91% (11)
- NCLEX Cram Sheet GuideDokument14 SeitenNCLEX Cram Sheet Guidecyberwong98% (66)
- Imm5788 2-U6dagko PDFDokument1 SeiteImm5788 2-U6dagko PDFJm CoguincoNoch keine Bewertungen
- Imm5788 2-U6dagko PDFDokument1 SeiteImm5788 2-U6dagko PDFJm CoguincoNoch keine Bewertungen
- Artifact Tierlist TableDokument7 SeitenArtifact Tierlist TableJm CoguincoNoch keine Bewertungen
- Articles: Use of A / An / TheDokument1 SeiteArticles: Use of A / An / TheJm CoguincoNoch keine Bewertungen
- Orthopedic Nursing. Lecture Notes at Philipine Orthopedic CenterDokument7 SeitenOrthopedic Nursing. Lecture Notes at Philipine Orthopedic Centerhannjazz100% (5)
- StudyGuide BurnsDokument2 SeitenStudyGuide BurnsJm CoguincoNoch keine Bewertungen
- Cami 9 BookDokument165 SeitenCami 9 BookThien LeNoch keine Bewertungen
- Cami 9 BookDokument165 SeitenCami 9 BookThien LeNoch keine Bewertungen
- Conceptual FrameworkDokument1 SeiteConceptual FrameworkJm CoguincoNoch keine Bewertungen
- Drugs!!!!Dokument7 SeitenDrugs!!!!Jm CoguincoNoch keine Bewertungen
- Abdominal Pain FinalDokument6 SeitenAbdominal Pain FinalJm CoguincoNoch keine Bewertungen
- Department of Health - Unang Yakap (Essential Newborn Care - Protocol For New Life) - 2012-03-27Dokument1 SeiteDepartment of Health - Unang Yakap (Essential Newborn Care - Protocol For New Life) - 2012-03-27daryl ann dep-asNoch keine Bewertungen
- Laboratory AnalysisDokument6 SeitenLaboratory AnalysisJm CoguincoNoch keine Bewertungen
- NCP HospicioDokument3 SeitenNCP HospicioJm CoguincoNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- National Cancer Control Program OverviewDokument15 SeitenNational Cancer Control Program OverviewAparna Kingini100% (1)
- Addis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaDokument21 SeitenAddis Ababa University: Collage of Health Science Pediatrics and Neonatology On PneumoniaCheru DugaseNoch keine Bewertungen
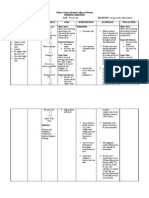
- Drug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDokument4 SeitenDrug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDan HizonNoch keine Bewertungen
- 2925 Ferose F 1415097720Dokument2 Seiten2925 Ferose F 1415097720iqbalmedicoNoch keine Bewertungen
- NHS LA - Duty of Candour 2014 - SlidesDokument10 SeitenNHS LA - Duty of Candour 2014 - SlidesAgnieszka WaligóraNoch keine Bewertungen
- Balanopostitis and Penyle Edema Atypical Manifestation of Primary SipilisDokument2 SeitenBalanopostitis and Penyle Edema Atypical Manifestation of Primary SipilisTeja LaksanaNoch keine Bewertungen
- Meniscus Disorders, Knee: The Medical Disability Advisor: Workplace Guidelines For Disability DurationDokument5 SeitenMeniscus Disorders, Knee: The Medical Disability Advisor: Workplace Guidelines For Disability DurationStephen Nathaniel100% (1)
- Notes Skin Eye Ears Infections MicrobioDokument18 SeitenNotes Skin Eye Ears Infections MicrobioChristiel John MagtibayNoch keine Bewertungen
- Lesson 20Dokument4 SeitenLesson 20Ananta KhanalNoch keine Bewertungen
- Modern Management of Anal FistulaDokument11 SeitenModern Management of Anal FistulaMayerlin CalvacheNoch keine Bewertungen
- Understanding Anemia: Causes, Symptoms, Diagnosis and TreatmentDokument27 SeitenUnderstanding Anemia: Causes, Symptoms, Diagnosis and Treatment1108010091Noch keine Bewertungen
- Hospitalized for Bleeding Peptic UlcerDokument53 SeitenHospitalized for Bleeding Peptic UlcerHoney Lyn AlebioNoch keine Bewertungen
- Policy For Exemption From Assessment and Examination FinalDokument28 SeitenPolicy For Exemption From Assessment and Examination FinalGloria JaisonNoch keine Bewertungen
- Hubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020Dokument6 SeitenHubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020nur halimaNoch keine Bewertungen
- Timing of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyDokument3 SeitenTiming of Antimicrobial Prophylaxis and Infectious Complications in Pediatric Patients Undergoing AppendicectomyJuan J. Acosta VelásquezNoch keine Bewertungen
- Conservative Management of Cutaneous Sinus Tract of Dental Origin Report of Two CasesDokument4 SeitenConservative Management of Cutaneous Sinus Tract of Dental Origin Report of Two CasesInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Severe Cutaneous Adverse Drug ReactionDokument87 SeitenSevere Cutaneous Adverse Drug ReactionEpi PanjaitanNoch keine Bewertungen
- 4 - Drug Product Design ParametersDokument7 Seiten4 - Drug Product Design ParametersVinz AlvarezNoch keine Bewertungen
- Region Name of LaboratoryDokument7 SeitenRegion Name of LaboratorySabling DritzcNoch keine Bewertungen
- Keywords:-URI, Infection, Respiratory System, STP,: Mothers, Under Five ChildrenDokument9 SeitenKeywords:-URI, Infection, Respiratory System, STP,: Mothers, Under Five ChildrenInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- A Comprehensive Introduction To Abdominal Acupuncture 1519537480Dokument5 SeitenA Comprehensive Introduction To Abdominal Acupuncture 1519537480Marco GutzNoch keine Bewertungen
- Table BDokument44 SeitenTable Bashwin katareNoch keine Bewertungen
- The Expanded Program On ImmunizationDokument26 SeitenThe Expanded Program On ImmunizationJudee Marie MalubayNoch keine Bewertungen
- Rinvoq Extended Release Tablets 15 MGDokument8 SeitenRinvoq Extended Release Tablets 15 MGMd Amdadul HoqueNoch keine Bewertungen
- Efektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumDokument8 SeitenEfektifitas Latihan Progressive Muscle Relaxation (PMR) Terhadap Mual Muntah Kemoterapi Pasien Kanker OvariumMutmin AnsariNoch keine Bewertungen
- 009the Automated Nucleated Red Cell Count On The Sysmex XE-2100Dokument5 Seiten009the Automated Nucleated Red Cell Count On The Sysmex XE-2100blanket_thNoch keine Bewertungen
- A Case Study of The Health CareDokument1 SeiteA Case Study of The Health CareJean LeongNoch keine Bewertungen
- Differential Diagnosis of Liver NoduleDokument46 SeitenDifferential Diagnosis of Liver NoduleJoydip SenNoch keine Bewertungen
- GE - MS Accessories GuideDokument50 SeitenGE - MS Accessories GuidemaruthaiNoch keine Bewertungen
- Minutes of Meeting November 2020Dokument2 SeitenMinutes of Meeting November 2020Jonella Anne CastroNoch keine Bewertungen