Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- DSM IIDokument136 SeitenDSM IIfarleyknight100% (17)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Mindfulness For Bipolar DisorderDokument218 SeitenMindfulness For Bipolar DisorderEmanuela Bartniski100% (4)
- Module 16 - Pharmacotherapy For Psychiatric DisordersDokument157 SeitenModule 16 - Pharmacotherapy For Psychiatric Disordersgeekay79Noch keine Bewertungen
- SAFE T Protocol W C SSRS and Columbia Risk and Protective Factors RecentDokument4 SeitenSAFE T Protocol W C SSRS and Columbia Risk and Protective Factors RecentCiupi TikNoch keine Bewertungen
- Substance Use Disorder Fact SheetDokument2 SeitenSubstance Use Disorder Fact SheetAnonymous nz9rhHNoch keine Bewertungen
- Overview of Somatoform DisordersDokument34 SeitenOverview of Somatoform DisordersmebibegNoch keine Bewertungen
- Case Analysis-Patty Duke PDFDokument13 SeitenCase Analysis-Patty Duke PDFRuth Ann CuerdoNoch keine Bewertungen
- Schizotypal Personality DisorderDokument6 SeitenSchizotypal Personality Disordercora4eva5699100% (1)
- Check Your ChildDokument33 SeitenCheck Your ChildBinod Narayan SethiNoch keine Bewertungen
- Draw A Person TestDokument3 SeitenDraw A Person TestLM CuestaNoch keine Bewertungen
- Behavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenDokument275 SeitenBehavioral Guide To Personality Disorders - (DSM-5) (2015) by Douglas H. RubenCristianBale100% (6)
- The Needs of Iranian Families of Children With Autism Spectrum Disorder, Cross-Cultural StudyDokument6 SeitenThe Needs of Iranian Families of Children With Autism Spectrum Disorder, Cross-Cultural StudyClaudiaClotanNoch keine Bewertungen
- Name: Anosha Khan (12562) Bba-H Webinar Reflection Report 2 Topic: Stress and Anxiety Management Campus: AirportDokument3 SeitenName: Anosha Khan (12562) Bba-H Webinar Reflection Report 2 Topic: Stress and Anxiety Management Campus: AirportAhsan MemonNoch keine Bewertungen
- Mental Health Powerpoint WeeblyDokument16 SeitenMental Health Powerpoint Weeblyapi-357279757Noch keine Bewertungen
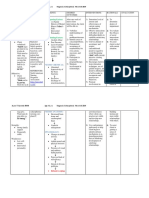
- Cognitive Behavioural Group Programme For Bipolar Affective DisorderDokument3 SeitenCognitive Behavioural Group Programme For Bipolar Affective DisorderAndreea PopaNoch keine Bewertungen
- The Numerb 23, SummaryDokument17 SeitenThe Numerb 23, SummaryFlora Angeli PastoresNoch keine Bewertungen
- Hypochondria 3 FormsDokument9 SeitenHypochondria 3 FormsYulianMitevNoch keine Bewertungen
- NCP 2nd PsychiaDokument4 SeitenNCP 2nd PsychiaLadymae CaberteNoch keine Bewertungen
- EBR No. 1 - Antepartum Duty (DERONIA)Dokument2 SeitenEBR No. 1 - Antepartum Duty (DERONIA)Chrizley Shawn DeroniaNoch keine Bewertungen
- Defensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsDokument2 SeitenDefensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsJeyser T. GamutiaNoch keine Bewertungen
- Disorder S: Corpuz, Rachella Nicole P. Spup Junior InternDokument53 SeitenDisorder S: Corpuz, Rachella Nicole P. Spup Junior InternRachella Nicole CorpuzNoch keine Bewertungen
- Weekly Record of Anxiety and Depression: 0 1 2 3 4 5 6 7 8 None Slight Moderate A Lot As Much As You Can ImagineDokument1 SeiteWeekly Record of Anxiety and Depression: 0 1 2 3 4 5 6 7 8 None Slight Moderate A Lot As Much As You Can ImagineMara_UriNoch keine Bewertungen
- Psychopathology NotesDokument29 SeitenPsychopathology Notesmonster40lbsNoch keine Bewertungen
- Mild Neurocognitive Disorder Fact Sheet PDFDokument1 SeiteMild Neurocognitive Disorder Fact Sheet PDFAle M. MartinezNoch keine Bewertungen
- Miles Francis 2014Dokument3 SeitenMiles Francis 2014Jorge RamírezNoch keine Bewertungen
- Post Concussion SyndromeDokument2 SeitenPost Concussion SyndromeCeleborn021100% (2)
- Antisocial Personality DisorderDokument9 SeitenAntisocial Personality Disordersandi_moore_1Noch keine Bewertungen
- Aspergers Syndrome Through The LifespanDokument8 SeitenAspergers Syndrome Through The LifespanAdnan Zaki BunyaminNoch keine Bewertungen
- Body Dysmorphic DisorderDokument5 SeitenBody Dysmorphic DisorderAnonymous I78Rzn6rS100% (1)
- Addiction EssayDokument5 SeitenAddiction Essayapi-341235528Noch keine Bewertungen