Das könnte Ihnen auch gefallen
- Synchronous Premaxillary Osteotomy With Primary.5Dokument8 SeitenSynchronous Premaxillary Osteotomy With Primary.5Angga PutraNoch keine Bewertungen
- Efek Supplen GlutaminDokument13 SeitenEfek Supplen GlutaminAngga PutraNoch keine Bewertungen
- Nasal Analysis and Anatomy: Anthropometric Proportional Assessment in Asians-Aesthetic Balance From Forehead To Chin, Part IDokument7 SeitenNasal Analysis and Anatomy: Anthropometric Proportional Assessment in Asians-Aesthetic Balance From Forehead To Chin, Part IAngga PutraNoch keine Bewertungen
- Mandibula 2Dokument13 SeitenMandibula 2Angga PutraNoch keine Bewertungen
- Wound Healing Animal Kawasumi2012Dokument17 SeitenWound Healing Animal Kawasumi2012Angga PutraNoch keine Bewertungen
- IcvDokument1 SeiteIcvAngga PutraNoch keine Bewertungen
- Wound Healing Animal Kawasumi2012Dokument17 SeitenWound Healing Animal Kawasumi2012Angga PutraNoch keine Bewertungen
- Amino Acid Supplementation and Impact OnDokument13 SeitenAmino Acid Supplementation and Impact OnISABELNoch keine Bewertungen
- Acinobakter 222Dokument4 SeitenAcinobakter 222Angga PutraNoch keine Bewertungen
- Local Glutamine Metabolism in Wounds and Inflammation: Michael D. CaldwellDokument6 SeitenLocal Glutamine Metabolism in Wounds and Inflammation: Michael D. CaldwellAngga PutraNoch keine Bewertungen
- Definisi dan Tatalaksana Awal Luka BakarDokument25 SeitenDefinisi dan Tatalaksana Awal Luka BakarAngga Putra Kusuma KusumaNoch keine Bewertungen
- Rhinoplasty: Surface Aesthetics and Surgical TechniquesDokument13 SeitenRhinoplasty: Surface Aesthetics and Surgical TechniquesAngga PutraNoch keine Bewertungen
- IcvDokument1 SeiteIcvAngga PutraNoch keine Bewertungen
- IcvDokument1 SeiteIcvAngga PutraNoch keine Bewertungen
- Lshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvDokument1 SeiteLshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvAngga PutraNoch keine Bewertungen
- 14 Anterolateral Thigh FlapDokument6 Seiten14 Anterolateral Thigh FlapAngga Putra100% (1)
- Lshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvDokument1 SeiteLshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvAngga PutraNoch keine Bewertungen
- Jsssssssssssssssssssssssssssssssssssssss Kaa B KDokument1 SeiteJsssssssssssssssssssssssssssssssssssssss Kaa B KAngga PutraNoch keine Bewertungen
- Prosedur Penerimaan PPDS Bedah PlastikDokument4 SeitenProsedur Penerimaan PPDS Bedah PlastikAngga PutraNoch keine Bewertungen
- Effect of NAC After Thermal InjuryDokument7 SeitenEffect of NAC After Thermal InjuryAngga PutraNoch keine Bewertungen
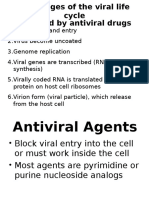
- Antiviral Acyclovir Pc2 DmsDokument5 SeitenAntiviral Acyclovir Pc2 DmsAngga PutraNoch keine Bewertungen
- Hand Injury Full TextDokument4 SeitenHand Injury Full TextAngga PutraNoch keine Bewertungen
- Departement of Anatomy Medical Faculty of North Sumatra UniversityDokument65 SeitenDepartement of Anatomy Medical Faculty of North Sumatra UniversityAngga PutraNoch keine Bewertungen
- E-Poster-Diagnostic in Hand Injury Before Operation, Does It Matter - For MergeDokument1 SeiteE-Poster-Diagnostic in Hand Injury Before Operation, Does It Matter - For MergeAngga PutraNoch keine Bewertungen
- Lower Extremity: Departement of Anatomy Medical Faculty of North Sumatera UtaraDokument23 SeitenLower Extremity: Departement of Anatomy Medical Faculty of North Sumatera UtaraAngga Putra100% (1)
- K-13 Lapkas OsteomyelitisDokument33 SeitenK-13 Lapkas OsteomyelitisAngga PutraNoch keine Bewertungen
- American Burn Association Practice GuidelinesDokument10 SeitenAmerican Burn Association Practice GuidelinesJosé María Llerena Otiniano100% (1)
- K-30, K-31 Kuliah FK Kista Dan InfeksiDokument43 SeitenK-30, K-31 Kuliah FK Kista Dan InfeksiAngga PutraNoch keine Bewertungen
- K-21 Miopati 2011Dokument70 SeitenK-21 Miopati 2011Angga PutraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Introduction to ImmunohematologyDokument16 SeitenIntroduction to ImmunohematologyJoshua TrinidadNoch keine Bewertungen
- Predictions Using Data Mining and Case Based Reasoning A Case Study For RetinopathyDokument4 SeitenPredictions Using Data Mining and Case Based Reasoning A Case Study For RetinopathyBiraj kumar BholNoch keine Bewertungen
- 23 ENT DiordersDokument114 Seiten23 ENT Diordersmohamed shamsNoch keine Bewertungen
- All Mycoses SGDDokument140 SeitenAll Mycoses SGDkashan100% (1)
- Anomalies of ConvergenceDokument12 SeitenAnomalies of ConvergenceDaniDenzongpaSulaemanNoch keine Bewertungen
- GERD Nursing CareDokument9 SeitenGERD Nursing CareTrisha ArizalaNoch keine Bewertungen
- Intubasi Sulit: Nur Hajriya BrahmiDokument26 SeitenIntubasi Sulit: Nur Hajriya BrahmiFathiah HusainNoch keine Bewertungen
- CLINICAL CHEMISTRY 2 Tumor MarkersDokument3 SeitenCLINICAL CHEMISTRY 2 Tumor MarkersSuzzaine EniazzusNoch keine Bewertungen
- Benazepril Hydrochloride (Drug Study)Dokument3 SeitenBenazepril Hydrochloride (Drug Study)Franz.thenurse6888100% (1)
- Chapter 4 Communicable DiseaseDokument33 SeitenChapter 4 Communicable DiseaseAyro Business CenterNoch keine Bewertungen
- Private Practice and Public School Speech Therapy Options in AustinDokument2 SeitenPrivate Practice and Public School Speech Therapy Options in Austiniese027Noch keine Bewertungen
- Maternal & Child Care Nursing Table of ContentsDokument2 SeitenMaternal & Child Care Nursing Table of Contentsɹǝʍdןnos100% (4)
- McGlamry's Forefoot SurgeryDokument629 SeitenMcGlamry's Forefoot SurgeryPourrielNoch keine Bewertungen
- Study DesignDokument130 SeitenStudy Designephremtigabie7Noch keine Bewertungen
- Ebp Picc Line - RevisedDokument6 SeitenEbp Picc Line - Revisedapi-234544335Noch keine Bewertungen
- The Impact of Good HealthDokument5 SeitenThe Impact of Good HealthavasiNoch keine Bewertungen
- Application of Recombinant DNADokument2 SeitenApplication of Recombinant DNANathan B. MhineNoch keine Bewertungen
- Health EducationDokument6 SeitenHealth EducationCakama MbimbiNoch keine Bewertungen
- NS Compounding Set 4 PDFDokument24 SeitenNS Compounding Set 4 PDFJulia BottiniNoch keine Bewertungen
- Risk Prediction Model for Heart Failure in DiabetesDokument20 SeitenRisk Prediction Model for Heart Failure in DiabetesjamesboendNoch keine Bewertungen
- HC09 ErgonomicsDokument29 SeitenHC09 ErgonomicsRegina LieNoch keine Bewertungen
- Comparing Phenol and Apamarg Kshar for Sclerotherapy in Bleeding PilesDokument8 SeitenComparing Phenol and Apamarg Kshar for Sclerotherapy in Bleeding PilesNishant SainiNoch keine Bewertungen
- Community Health Nursing Compre.2015with RatioDokument8 SeitenCommunity Health Nursing Compre.2015with RatioAndrea BroccoliNoch keine Bewertungen
- Brain 101 Info (Merged) PDFDokument186 SeitenBrain 101 Info (Merged) PDFrosyuaNoch keine Bewertungen
- Career Map - DoctorDokument7 SeitenCareer Map - DoctorAdityaNoch keine Bewertungen
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDokument9 SeitenUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerNoch keine Bewertungen
- Differences Between T.solium and T.saginata: Taeniasis or CysticercosisDokument3 SeitenDifferences Between T.solium and T.saginata: Taeniasis or CysticercosisVenkatapradeepNoch keine Bewertungen
- Review Article: Guided Bone Regeneration: A Literature ReviewDokument16 SeitenReview Article: Guided Bone Regeneration: A Literature ReviewGonçalo Gomes SanchesNoch keine Bewertungen
- Toacs 5Dokument244 SeitenToacs 5Mobin Ur Rehman Khan100% (2)
- Muhammad YounasDokument4 SeitenMuhammad YounasHamid IqbalNoch keine Bewertungen