Das könnte Ihnen auch gefallen
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- GlaucomaDokument42 SeitenGlaucomaMaryTanNoch keine Bewertungen
- Glaucoma: Seminar OnDokument43 SeitenGlaucoma: Seminar OnSanjay GarasiyaNoch keine Bewertungen
- Disorders of The EyeDokument16 SeitenDisorders of The Eyelisette_sakuraNoch keine Bewertungen
- About 70% of All Sensory Information Reaches The Brain Through The EyesDokument127 SeitenAbout 70% of All Sensory Information Reaches The Brain Through The Eyesjoan olanteNoch keine Bewertungen
- Glaucoma Case StudyDokument5 SeitenGlaucoma Case StudyEdgel QuidolesNoch keine Bewertungen
- Glaucoma Presentation - Information, Risk Factors and DetectionDokument29 SeitenGlaucoma Presentation - Information, Risk Factors and DetectionAlina Lagoviyer100% (11)
- Glaucoma Word FileDokument34 SeitenGlaucoma Word Fileanon_784834955100% (1)
- CataractDokument35 SeitenCataractyusufharkianNoch keine Bewertungen
- ConjunctivitisDokument5 SeitenConjunctivitisAmrit Preet KaurNoch keine Bewertungen
- HyperopiaDokument6 SeitenHyperopiaTesfsh MekonenNoch keine Bewertungen
- CataractDokument6 SeitenCataractSairileenDoradoNoch keine Bewertungen
- Hyphema 2Dokument7 SeitenHyphema 2heidyNoch keine Bewertungen
- CataractDokument7 SeitenCataractNader Smadi100% (2)
- Ptosis Types & Clinical Features: Made By:-Amritansh PandeyDokument14 SeitenPtosis Types & Clinical Features: Made By:-Amritansh PandeyalexNoch keine Bewertungen
- Retinal DetachmentDokument16 SeitenRetinal DetachmentCandice Lim Swee LingNoch keine Bewertungen
- Burns: College of NursingDokument12 SeitenBurns: College of NursingAyr Masenas100% (1)
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniDokument46 SeitenCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniNoch keine Bewertungen
- CataractDokument5 SeitenCataractcarls burg a. resurreccionNoch keine Bewertungen
- CATARACTS and GLAUCOMADokument11 SeitenCATARACTS and GLAUCOMAAmoroso, Marian Corneth D.Noch keine Bewertungen
- Addisonian Crisis: Manish K Medical Officer IgmhDokument47 SeitenAddisonian Crisis: Manish K Medical Officer IgmhNaaz Delhiwale100% (1)
- Neurogenic Shock (New)Dokument14 SeitenNeurogenic Shock (New)Syarafina AminuddinNoch keine Bewertungen
- Running Head: A Patient Who Has Glaucoma 1Dokument10 SeitenRunning Head: A Patient Who Has Glaucoma 1Alonso LugoNoch keine Bewertungen
- BlepharitisDokument20 SeitenBlepharitisNorshahidah IedaNoch keine Bewertungen
- By: Noor Majeed RehaniDokument23 SeitenBy: Noor Majeed RehaniMihaela Toma0% (1)
- WILMs TumorDokument3 SeitenWILMs TumorLorie May GuillangNoch keine Bewertungen
- Glaucoma 180813151731Dokument24 SeitenGlaucoma 180813151731malathiNoch keine Bewertungen
- PanophthalmitisDokument31 SeitenPanophthalmitisRizty Mayang FachleviNoch keine Bewertungen
- CATARACTSDokument2 SeitenCATARACTSHanee Kaye TagubaNoch keine Bewertungen
- Cataract InformationDokument25 SeitenCataract Informationvasanth_1515Noch keine Bewertungen
- Ophthalmic EmergencyDokument17 SeitenOphthalmic EmergencyMohammad HelalNoch keine Bewertungen
- Pemphigus vulgarisPPTDokument23 SeitenPemphigus vulgarisPPTSiti HanisaNoch keine Bewertungen
- CATARACTDokument15 SeitenCATARACTCharmilli PotestasNoch keine Bewertungen
- Eye ExaminationDokument23 SeitenEye Examinationcynthia167Noch keine Bewertungen
- CraniotomyDokument8 SeitenCraniotomySyed AbudaheerNoch keine Bewertungen
- Multiple SclerosisDokument6 SeitenMultiple SclerosisRonnel Alvin Antonio AdrianoNoch keine Bewertungen
- BLEPHARITISDokument25 SeitenBLEPHARITISSrijana MahatoNoch keine Bewertungen
- Retinal DetachmentDokument8 SeitenRetinal DetachmentMaisarah BakariNoch keine Bewertungen
- ShockDokument21 SeitenShockMin-Joo Esther ParkNoch keine Bewertungen
- Cataract NewDokument51 SeitenCataract NewApoorva AgrawalNoch keine Bewertungen
- PancreatitisDokument59 SeitenPancreatitisAarif RanaNoch keine Bewertungen
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dokument70 SeitenPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNoch keine Bewertungen
- CellulitisDokument15 SeitenCellulitisSujatha J JayabalNoch keine Bewertungen
- Glaucoma: Zarieh Dawn Novela Medicine 2Dokument41 SeitenGlaucoma: Zarieh Dawn Novela Medicine 2Zari NovelaNoch keine Bewertungen
- Pathophysiology of Pain and Pain Assessment PDFDokument12 SeitenPathophysiology of Pain and Pain Assessment PDFRaisa AriesthaNoch keine Bewertungen
- HydronephrosisDokument17 SeitenHydronephrosisShradha Khurana100% (1)
- Brain Tumor PDFDokument11 SeitenBrain Tumor PDFSujith KuttanNoch keine Bewertungen
- CataractDokument3 SeitenCataractShereen ManabilangNoch keine Bewertungen
- GlaucomaDokument31 SeitenGlaucomaJake Albert MiguelNoch keine Bewertungen
- Muscle Strength TestingDokument3 SeitenMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Rheumatoid ArthritisDokument4 SeitenRheumatoid Arthritisapi-3822433Noch keine Bewertungen
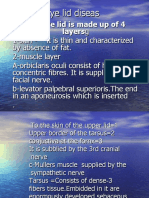
- The EyelidsDokument64 SeitenThe EyelidsSarahNoch keine Bewertungen
- Paget's DiseaseDokument24 SeitenPaget's DiseaseKim Gonzales100% (5)
- Nursing Assessment S - O Pt. May ManifestDokument4 SeitenNursing Assessment S - O Pt. May Manifestk_a1990Noch keine Bewertungen
- Cataract: Done by Jony MallikDokument46 SeitenCataract: Done by Jony MallikAlfa Suryani ArdliNoch keine Bewertungen
- Aqueous HumorDokument46 SeitenAqueous HumorJ NATASHA MARIANoch keine Bewertungen
- Eye Lid DiseasDokument59 SeitenEye Lid DiseasJohanna Tania PriatoNoch keine Bewertungen
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDokument2 SeitenPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenNoch keine Bewertungen
- ConjunctivitisDokument18 SeitenConjunctivitisPrashanth Padmini VenugopalNoch keine Bewertungen
- Summit College NCLEX LECTURE NOTES VIDEO 1-11Dokument98 SeitenSummit College NCLEX LECTURE NOTES VIDEO 1-11plethoraldork90% (20)
- Final OSCE Script 220117Dokument18 SeitenFinal OSCE Script 220117plethoraldorkNoch keine Bewertungen
- Nursing ProcessDokument62 SeitenNursing ProcessplethoraldorkNoch keine Bewertungen
- Av FistulaDokument1 SeiteAv FistulaplethoraldorkNoch keine Bewertungen
- CBT Study GuideDokument10 SeitenCBT Study Guideplethoraldork100% (5)
- Management of The EVDDokument7 SeitenManagement of The EVDplethoraldork100% (1)
- Accreditation Requirements HemodialysisDokument12 SeitenAccreditation Requirements HemodialysisplethoraldorkNoch keine Bewertungen
- Stroke Guidelines: Cva Critical Pathway Department of NeurologyDokument5 SeitenStroke Guidelines: Cva Critical Pathway Department of NeurologyplethoraldorkNoch keine Bewertungen
- Vascular Access HemodialysisDokument19 SeitenVascular Access Hemodialysisplethoraldork100% (1)
- Ao2012-0001 New Rules & Regulations Governing The Licensing & Regulation of Dialysis Facilities in The Phils PDFDokument41 SeitenAo2012-0001 New Rules & Regulations Governing The Licensing & Regulation of Dialysis Facilities in The Phils PDFplethoraldorkNoch keine Bewertungen
- Key Scientific PublicationsDokument7 SeitenKey Scientific PublicationsplethoraldorkNoch keine Bewertungen
- Hemodialysis Accreditation RequirementsDokument13 SeitenHemodialysis Accreditation RequirementsplethoraldorkNoch keine Bewertungen
- Multiple SclerosisDokument2 SeitenMultiple Sclerosisplethoraldork100% (5)
- Cerebrovascular AccidentDokument8 SeitenCerebrovascular Accidentplethoraldork100% (10)
- Philippine Patient's Bill of RightsDokument6 SeitenPhilippine Patient's Bill of Rightsplethoraldork98% (49)
- Labor and DeliveryDokument7 SeitenLabor and Deliveryplethoraldork100% (20)
- Peritoneal DialysisDokument45 SeitenPeritoneal DialysisYum CNoch keine Bewertungen
- Template PPT BedahDokument51 SeitenTemplate PPT BedahHenry PrawiraNoch keine Bewertungen
- Pneumonia Template 1Dokument1 SeitePneumonia Template 1洪靖儀Noch keine Bewertungen
- PL - 730.4 - Ogd (Gastroscopy)Dokument12 SeitenPL - 730.4 - Ogd (Gastroscopy)Pontharani MarimuthuNoch keine Bewertungen
- Shaft of Tibia FracturesDokument38 SeitenShaft of Tibia FracturesSahithya MNoch keine Bewertungen
- Eustachian Tube DysfunctionDokument2 SeitenEustachian Tube DysfunctionAngela Mitchelle NyanganNoch keine Bewertungen
- Case StudyDokument11 SeitenCase StudyBounna PhoumalavongNoch keine Bewertungen
- Influenza Med Exemption Template 2014Dokument1 SeiteInfluenza Med Exemption Template 2014Alexander ChamessianNoch keine Bewertungen
- Carpal Tunnel SyndromeDokument3 SeitenCarpal Tunnel SyndromeAnonymous uTEAEbugNoch keine Bewertungen
- Pre-Diabetes:: Don't Let It Lead To Type-2Dokument1 SeitePre-Diabetes:: Don't Let It Lead To Type-2ARIA MINDNoch keine Bewertungen
- 2003 LG Nefropatia DiabeticaDokument13 Seiten2003 LG Nefropatia DiabeticaDario ToschiNoch keine Bewertungen
- Case Study On Normal Vaginal DeliveryDokument40 SeitenCase Study On Normal Vaginal DeliveryPabhat Kumar100% (1)
- 3 February 2010Dokument14 Seiten3 February 2010MasterFul5005Noch keine Bewertungen
- Torn MeniscusDokument10 SeitenTorn MeniscusKrystal Veverka100% (3)
- Blood Pressure MeasurementDokument27 SeitenBlood Pressure MeasurementArun rNoch keine Bewertungen
- Homeopathic Treatment of Cervical SpondylosisDokument9 SeitenHomeopathic Treatment of Cervical SpondylosisRobertBellarmineNoch keine Bewertungen
- 3i CatalogDokument79 Seiten3i CatalogJulie HollowayNoch keine Bewertungen
- 1 QuestionnaireDokument2 Seiten1 QuestionnaireHansgebiebcheNoch keine Bewertungen
- Cayabyab, Natasha Alaine E BSN Iv-E2Dokument3 SeitenCayabyab, Natasha Alaine E BSN Iv-E2Natasha Alaine E. CayabyabNoch keine Bewertungen
- NS Camp 2012 - Health History Form For HTsDokument1 SeiteNS Camp 2012 - Health History Form For HTsThanhThao NguyenNoch keine Bewertungen
- Pharmaceutical Care in Renal DiseaseDokument15 SeitenPharmaceutical Care in Renal DiseaseEfraim MangalukNoch keine Bewertungen
- Removal of Impacted Third MolarDokument13 SeitenRemoval of Impacted Third MolarHarkanNoch keine Bewertungen
- Olecranon Bursitis: DR VVR Choudhary MPT (Ortho) - SvimsDokument27 SeitenOlecranon Bursitis: DR VVR Choudhary MPT (Ortho) - Svimsvenkata ramakrishnaiahNoch keine Bewertungen
- Bala Murugan E - , MSC Nursing AIIMSDokument33 SeitenBala Murugan E - , MSC Nursing AIIMSBalaMuruganNoch keine Bewertungen
- Sleep Position WaiverDokument0 SeitenSleep Position WaiverAmanda's GardenNoch keine Bewertungen
- Sleep Questionnaire EnglishDokument5 SeitenSleep Questionnaire EnglishNazir AhmadNoch keine Bewertungen
- Spina Bifida OCCULTADokument1 SeiteSpina Bifida OCCULTArebelswanteddot_comNoch keine Bewertungen
- Vi. Ûrxm: ®vôtôw ® Øû/LsDokument4 SeitenVi. Ûrxm: ®vôtôw ® Øû/Lsbgk_usNoch keine Bewertungen
- Pacemaker After CareDokument4 SeitenPacemaker After CarePrasoon PremrajNoch keine Bewertungen
- LD IV InfusionDokument70 SeitenLD IV InfusionAbbeygale Galan100% (1)