Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Vignesh Ram HSE ResumeDokument3 SeitenVignesh Ram HSE ResumeTFattahNoch keine Bewertungen
- Student Development Theory Autobiography FinalDokument10 SeitenStudent Development Theory Autobiography Finalapi-541684468Noch keine Bewertungen
- 3GPP - Ts 36.133Dokument2.389 Seiten3GPP - Ts 36.133Kevin NightNoch keine Bewertungen
- DR ShekhawatDokument3 SeitenDR ShekhawatNittin Baru0% (2)
- Authoritarian Regimes: Gabriela Gonzalez VaillantDokument4 SeitenAuthoritarian Regimes: Gabriela Gonzalez VaillantLucan FlorentinaNoch keine Bewertungen
- Event Proposal Anukaran: Group-2Dokument9 SeitenEvent Proposal Anukaran: Group-2Srijan SaxenaNoch keine Bewertungen
- Your Great Escape: Sambo'S FarmDokument2 SeitenYour Great Escape: Sambo'S FarmSharmin ReulaNoch keine Bewertungen
- Literature Review On Job Satisfaction Among EmployeesDokument43 SeitenLiterature Review On Job Satisfaction Among EmployeesUrmila Mukundan67% (12)
- Service Strategy: Sachin Modgil IMI-KDokument44 SeitenService Strategy: Sachin Modgil IMI-KHarsh VivekNoch keine Bewertungen
- NDA TemplateDokument7 SeitenNDA Templatecrosalejos100% (1)
- Disappear Varsity WorkbookDokument12 SeitenDisappear Varsity WorkbooktortdogNoch keine Bewertungen
- CCN Mod 1Dokument67 SeitenCCN Mod 1LikithaReddy YenumulaNoch keine Bewertungen
- Kayla Green - Research Paper Draft 1 - Pages 1-3 Include Your Works Cited PageDokument7 SeitenKayla Green - Research Paper Draft 1 - Pages 1-3 Include Your Works Cited Pageapi-458133015Noch keine Bewertungen
- GPPAQ - PDF VersionDokument1 SeiteGPPAQ - PDF VersionEmma GundryNoch keine Bewertungen
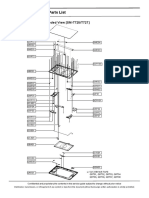
- Exploded View and Parts ListDokument2 SeitenExploded View and Parts ListVietmobile PageNoch keine Bewertungen
- Preventive Actions of Police: A Project Proposal Made byDokument23 SeitenPreventive Actions of Police: A Project Proposal Made bynupur jhodNoch keine Bewertungen
- Motion For TRODokument10 SeitenMotion For TROMarianne MartinezNoch keine Bewertungen
- 5 Cat Tools That Every Translator Should Use: 1. Translation Memory SoftwareDokument2 Seiten5 Cat Tools That Every Translator Should Use: 1. Translation Memory SoftwareYounes Y YounesNoch keine Bewertungen
- Marlins 2 Unit 7. Page 7.1 To 7.3Dokument3 SeitenMarlins 2 Unit 7. Page 7.1 To 7.3Kevindo SianiparNoch keine Bewertungen
- Individual Activity #3 - BullecerDokument2 SeitenIndividual Activity #3 - BullecerAbe Miguel BullecerNoch keine Bewertungen
- ResearchDokument7 SeitenResearchMars San CarlosNoch keine Bewertungen
- Third QuarterDokument4 SeitenThird QuarterNova Shielna A.MaglasangNoch keine Bewertungen
- Learning Styles of Social Studies 4th YearDokument14 SeitenLearning Styles of Social Studies 4th YearChristian AlfornonNoch keine Bewertungen
- TFN Notes 2ND LESSONDokument5 SeitenTFN Notes 2ND LESSONAlisa FujibayashiNoch keine Bewertungen
- LIVRO Following The Flows of Process A New MatDokument254 SeitenLIVRO Following The Flows of Process A New MatBeatriz SilvaNoch keine Bewertungen
- Financial Accounting Part 1Dokument7 SeitenFinancial Accounting Part 1Hazel Ranola VelosoNoch keine Bewertungen
- Abhishek GuptaDokument7 SeitenAbhishek GuptaAbhishek GuptaNoch keine Bewertungen
- Ayjnihh-Mum@nic inDokument21 SeitenAyjnihh-Mum@nic innileshmsawantNoch keine Bewertungen
- Final Coaching LeaDokument510 SeitenFinal Coaching LeaMatias Winner100% (3)
- Sam Rao ResumeDokument1 SeiteSam Rao ResumeAmitabh RaoNoch keine Bewertungen